

Key Strategies for Clinical Management and Improvement of Healthcare Services for Cardiovascular Disease and Diabetes Patients in the Coronavirus (COVID-19) Settings: Recommendations From the REPROGRAM Consortium
- PMID: 32613010
- PMCID: PMC7308556
- DOI: 10.3389/fcvm.2020.00112
Key Strategies for Clinical Management and Improvement of Healthcare Services for Cardiovascular Disease and Diabetes Patients in the Coronavirus (COVID-19) Settings: Recommendations From the REPROGRAM Consortium
Abstract
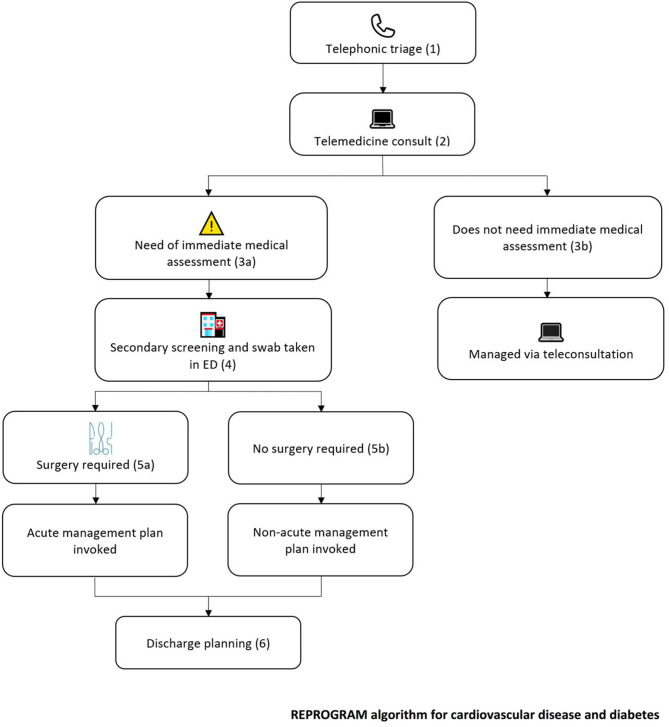
Patients with cardiovascular disease and diabetes are at potentially higher risk of infection and fatality due to COVID-19. Given the social and economic costs associated with disability due to these conditions, it is imperative that specific considerations for clinical management of these patients be observed. Moreover, the reorganization of health services around the pandemic response further exacerbates the growing crisis around limited access, treatment compliance, acute medical needs, and mental health of patients in this specific subgroup. Existing recommendations and guidelines emanating from respective bodies have addressed some of the pressure points; however, there are variations and limitations vis a vis patient with multiple comorbidities such as obesity. This article will pull together a comprehensive assessment of the association of cardiovascular disease, diabetes, obesity and COVID-19, its impact on the health systems and how best health systems can respond to mitigate current challenges and future needs. We anticipate that in the context of this pandemic, the cardiovascular disease and diabetes patients need a targeted strategy to ensure the harm to this group does not translate to huge costs to society and to the economy. Finally, we propose a triage and management protocol for patients with cardiovascular disease and diabetes in the COVID-19 settings to minimize harm to patients, health systems and healthcare workers alike.
Keywords: cardiovascular diseases (CVDs); clinical algorithm; coronavirus disease 2019 (COVID-19); diabetes; healthcare services; obesity; personal protective equipment (PPE).
Copyright © 2020 Bhaskar, Rastogi, Chattu, Adisesh, Thomas, Alvarado, Riahi, Varun, Pai, Barsam and Walker.
Figures
References
-
- John Hopkins University COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE). Johns Hopkins University; (2020). Available online at: https://coronavirus.jhu.edu/map.html (accessed April 6, 2020).
LinkOut - more resources
Full Text Sources