

Management of spinal deformities and tibial pseudarthrosis in children with neurofibromatosis type 1 (NF-1)
- PMID: 32613421
- PMCID: PMC8346390
- DOI: 10.1007/s00381-020-04775-4
Management of spinal deformities and tibial pseudarthrosis in children with neurofibromatosis type 1 (NF-1)
Erratum in
-
Correction to: Management of spinal deformities and tibial pseudarthrosis in children with neurofibromatosis type 1 (NF-1).Childs Nerv Syst. 2021 Oct;37(10):3281. doi: 10.1007/s00381-021-05303-8. Childs Nerv Syst. 2021. PMID: 34482418 Free PMC article. No abstract available.
Abstract
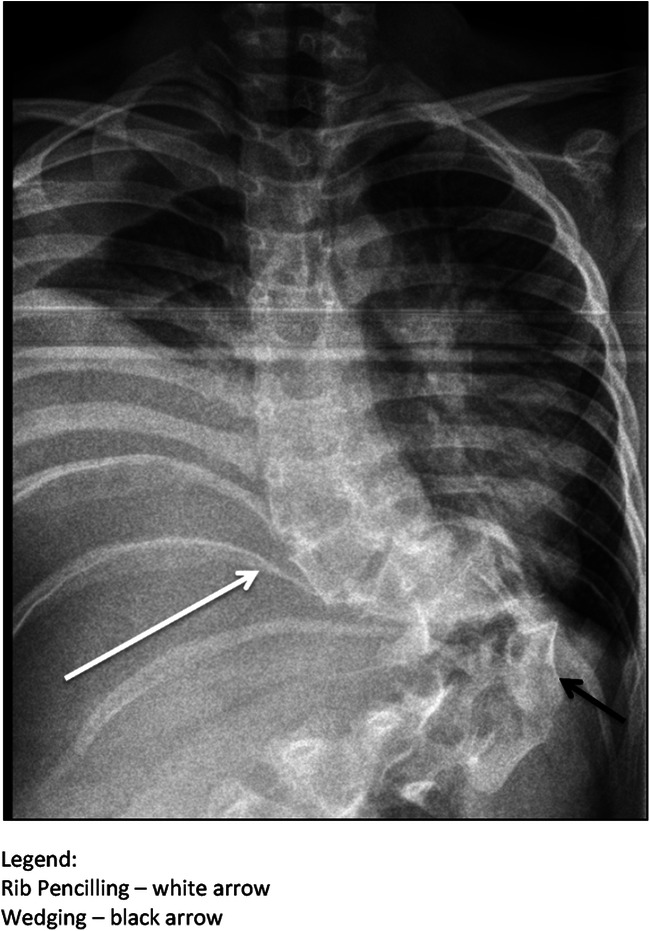
The skeletal system is affected in up to 60% of patients with neurofibromatosis type 1. The most commonly observed entities are spinal deformities and tibial dysplasia. Early recognition of radiologic osseous dystrophy signs is of utmost importance because worsening of the deformities without treatment is commonly observed and surgical intervention is often necessary. Due to the relative rarity and the heterogenic presentation of the disease, evidence regarding the best surgical strategy is still lacking.
Purpose: To report our experience with the treatment of skeletal manifestations in pediatric patients with (neurofibromatosis type 1) NF-1 and to present the results with our treatment protocols.
Materials and methods: This is a retrospective, single expert center study on children with spinal deformities and tibial dysplasia associated with NF-1 treated between 2006 and 2020 in a tertiary referral institution.
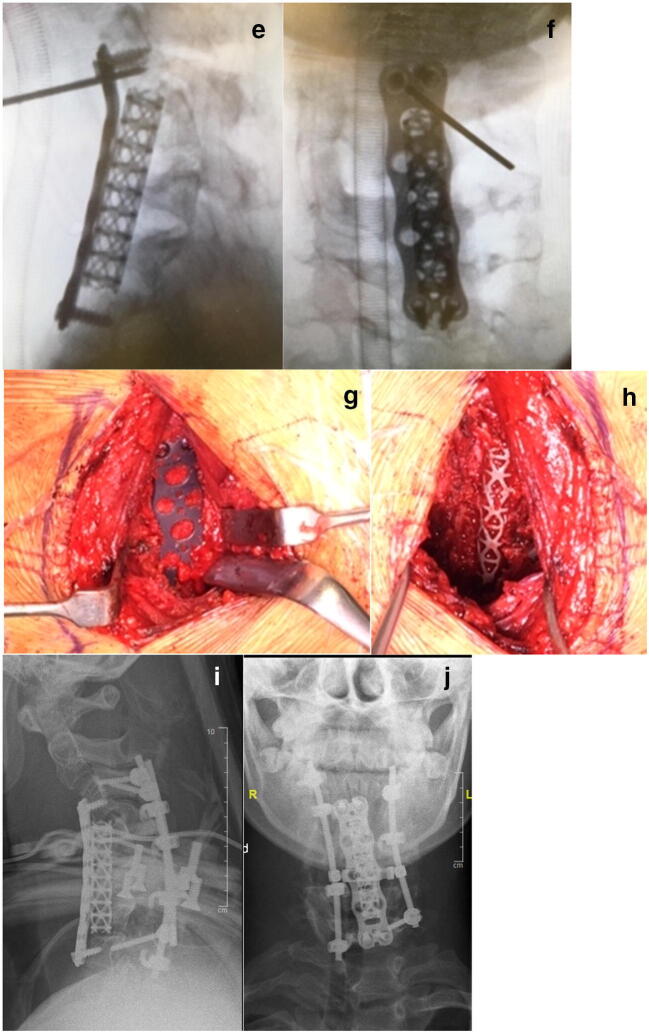
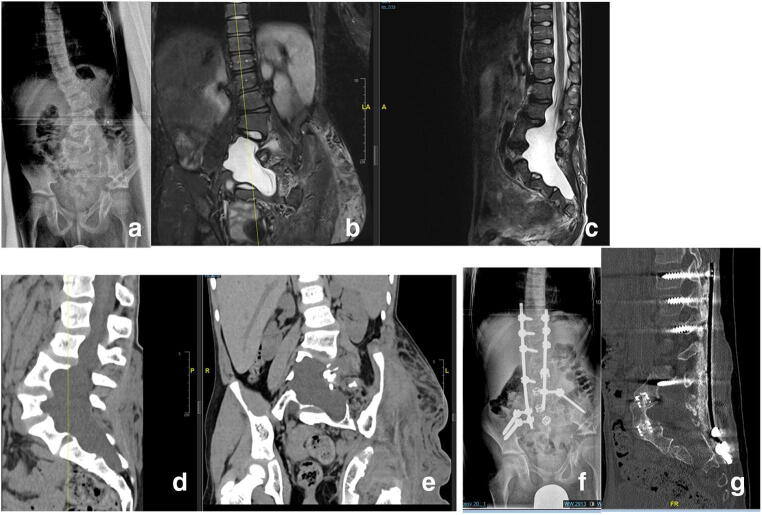
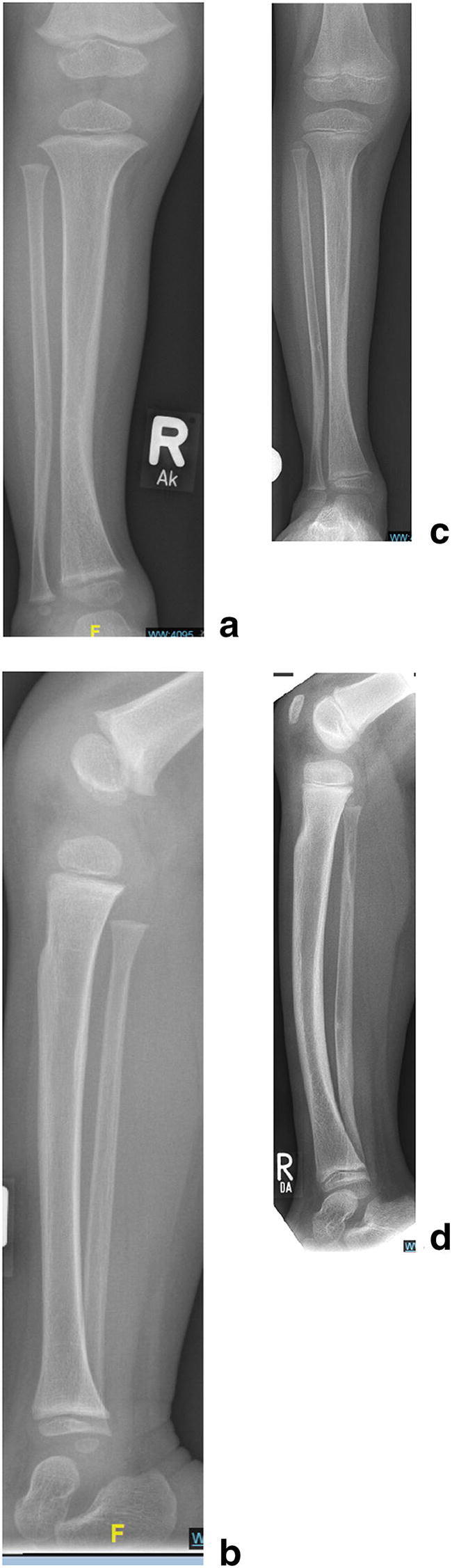
Results: Spinal deformity: Thirty-three patients (n = 33) were included. Mean age at index surgery was 9.8 years. In 30 patients (91%), the deformity was localized in the thoracic and/or lumbar spine, and in 3 patients (9%), there was isolated involvement of the cervical spine. Eleven patients (33%) received definitive spinal fusion as an index procedure and 22 (67%) were treated by means of "growth-preserving" spinal surgery. Halo-gravity traction before index surgery was applied in 11 patients (33%). Progression of deformity was stopped in all patients and a mean curve correction of 60% (range 23-98%) was achieved. Mechanical problems with instrumentation requiring revision surgery were observed in 55% of the patients treated by growth-preserving techniques and in none of the patients treated by definitive fusion. One patient (3%) developed a late incomplete paraplegia due to a progressive kyphotic deformity. Tibial dysplasia: The study group comprised of 14 patients. In 5 of them (36%) pathological fractures were present on initial presentation. In the remaining 9 patients (64%), anterior tibial bowing without fracture was observed initially. Four of them (n = 4, 28%) subsequently developed a pathologic fracture despite brace treatment. Surgical treatment was indicated in 89% of the children with pathological fractures. This involved resection of the pseudarthrosis, autologous bone grafting, and intramedullary nailing combined with external fixation in some of the cases. In 50% of the patients, bone morphogenic protein was used "off-label" in order to promote union. Healing of the pseudarthrosis was achieved in all of the cases and occurred between 5 to 13 months after the index surgical intervention. Four of the patients treated surgically needed more than one surgical intervention in order to achieve union; one patient had a re-fracture. All patients had a good functional result at last follow-up.
Conclusion: Early surgical intervention is recommended for the treatment dystrophic spinal deformity in children with NF-1. Good and sustainable curve correction without relevant thoracic growth inhibition can be achieved with growth-preserving techniques alone or in combination with short spinal fusion at the apex of the curve. Preoperative halo-gravity traction is a safe and very effective tool for the correction of severe and rigid deformity in order to avoid neurologic injury. Fracture union in tibial dysplasia with satisfactory functional results can be obtained in over 80% of the children by means of surgical resection of the pseudarthrosis, intramedullary nailing, and bone grafting. Wearing a brace until skeletal maturity is achieved is mandatory in order to minimize the risk of re-fracture.
Keywords: Congenital pseudarthrosis of the tibia; Dystrophic scoliosis; Neurofibromatosis type 1.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures








References
-
- Young-Hing K, Kalamchi A, MacEwen GD. Cervical spine abnormalities in neurofibromatosis. J Bone Joint Surg Am. 1979;61:659–659. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
