

Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation
- PMID: 32614258
- PMCID: PMC7336751
- DOI: 10.1148/radiol.2020202352
Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation
Abstract
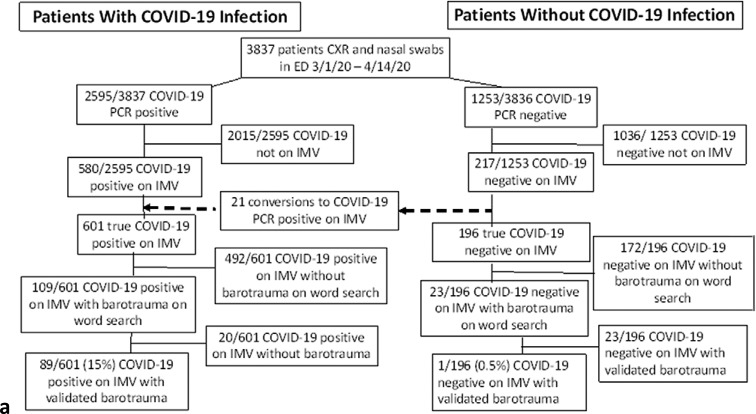
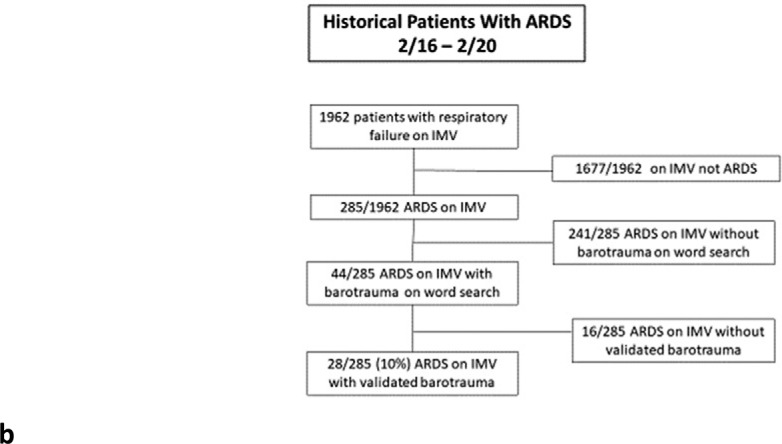
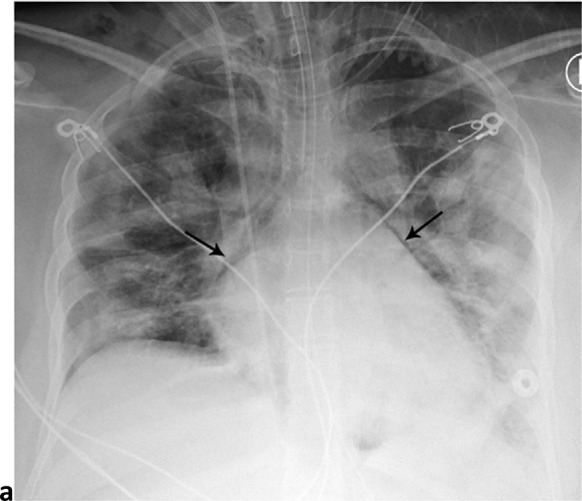
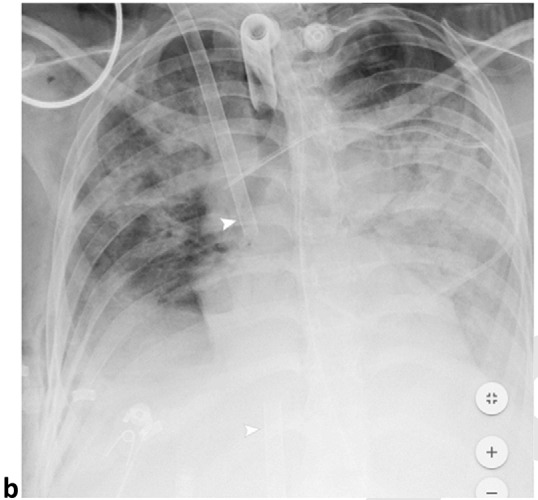
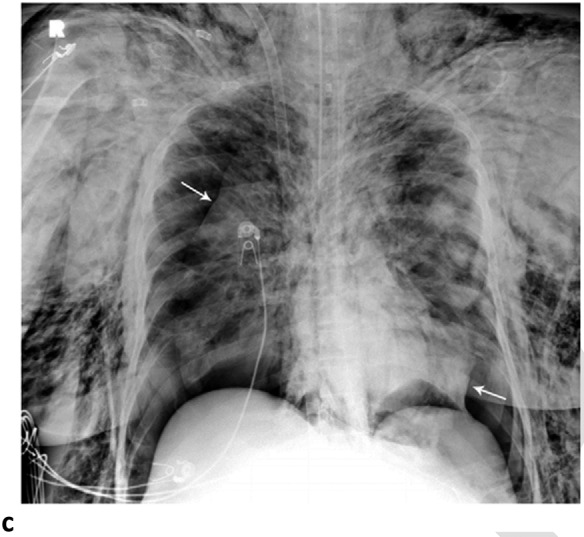
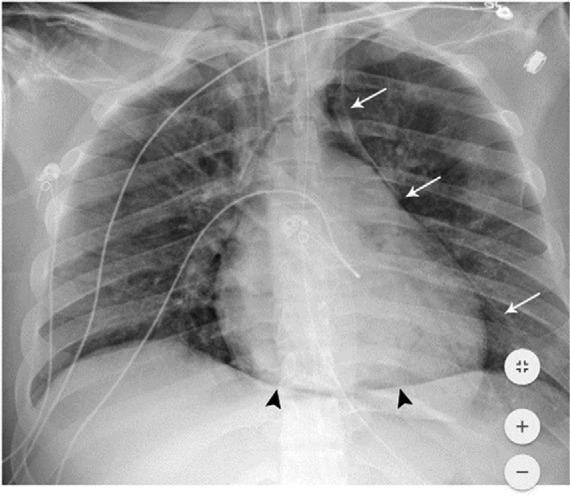
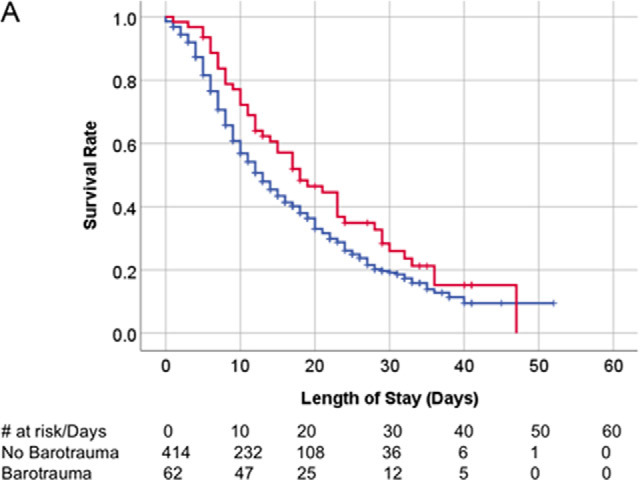
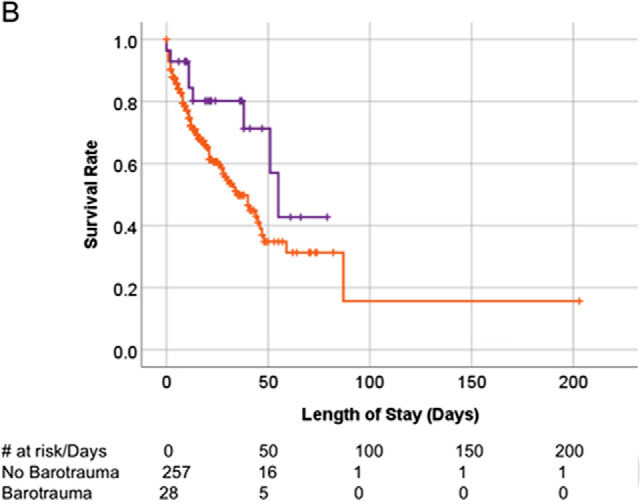
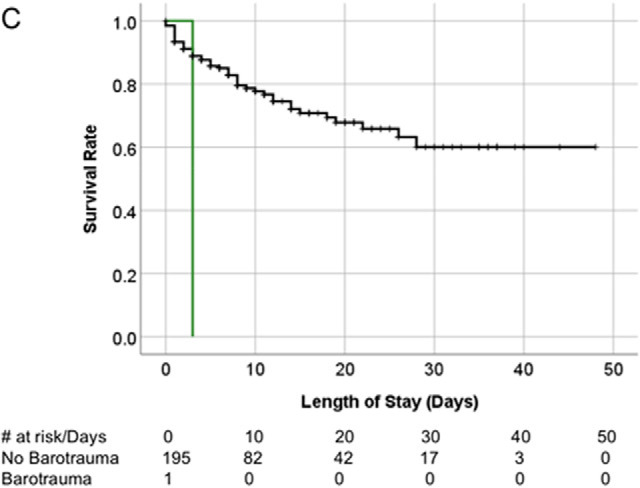
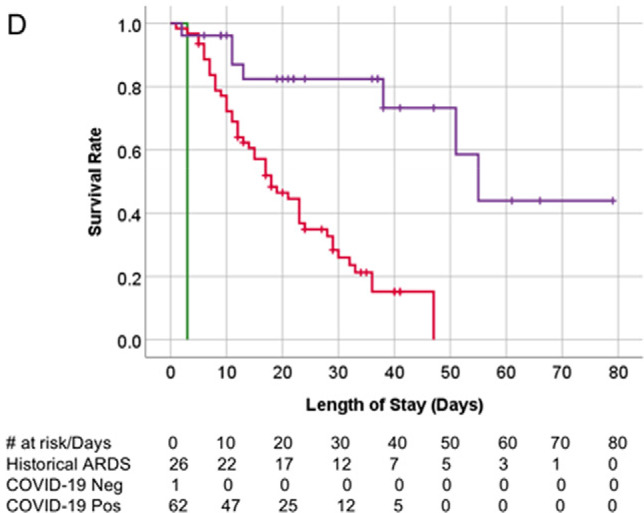
Background A high number of patients with coronavirus disease 2019 (COVID-19) pneumonia who had barotrauma related to invasive mechanical ventilation at the authors' institution were observed. Purpose To determine if the rate of barotrauma in patients with COVID-19 infection was greater than in other patients requiring invasive mechanical ventilation at the authors' institution. Materials and Methods In this retrospective study, clinical and imaging data of patients seen between March 1, 2020, and April 6, 2020, who tested positive for COVID-19 and experienced barotrauma associated with invasive mechanical ventilation, were compared with patients without COVID-19 infection during the same period. Historical comparison was made to barotrauma rates of patients with acute respiratory distress syndrome from February 1, 2016, to February 1, 2020, at the authors' institution. Comparison of patient groups was performed using categoric or continuous statistical testing as appropriate, with multivariable regression analysis. Patient survival was assessed using Kaplan-Meier curves analysis. Results A total of 601 patients with COVID-19 infection underwent invasive mechanical ventilation (mean age, 63 years ± 15 [standard deviation]; 71% men). Of the total, there were 89 (15%) patients with one or more barotrauma events for a total of 145 barotrauma events (24% overall events) (95% confidence interval [CI]: 21%, 28%). During the same period, 196 patients without COVID-19 infection (mean age, 64 years ± 19; 52% men) with invasive mechanical ventilation had one barotrauma event (0.5%; 95% CI: 0%, 3%; P < .001 vs the group with COVID-19 infection). Of 285 patients with acute respiratory distress syndrome on invasive mechanical ventilation during the previous 4 years (mean age, 68 years ± 17; 60% men), 28 patients (10%) had 31 barotrauma events, with an overall barotrauma rate of 11% (95% CI: 8%, 15%; P < .001 vs the group with COVID-19 infection). Barotrauma is an independent risk factor for death in COVID-19 (odds ratio = 2.2; P = .03) and is associated with a longer hospital stay (odds ratio = 0.92; P < .001). Conclusion Patients with coronavirus disease 2019 (COVID-19) infection and invasive mechanical ventilation had a higher rate of barotrauma than patients with acute respiratory distress syndrome and patients without COVID-19 infection. © RSNA, 2020 Online supplemental material is available for this article.
Figures
References
-
- Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospitalization and critical illness among 4,103 patients with COVID-19 disease in New York City. medRxiv. 2020:2020.2004.2008.20057794. Accepted for publication, British Journal of Medicine 2020
-
- Anzueto A, Frutos–Vivar F, Esteban A, et al. Incidence, risk factors and outcome of barotrauma in mechanically ventilated patients. Intensive care medicine. 2004;30(4):612-619. - PubMed
-
- Boussarsar M, Thierry G, Jaber S, Roudot-Thoraval F, Lemaire F, Brochard L. Relationship between ventilatory settings and barotrauma in the acute respiratory distress syndrome. Intensive care medicine. 2002;28(4):406-413. - PubMed
-
- Briel M, Meade M, Mercat A, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. Jama. 2010;303(9):865-873. - PubMed
-
- Grasso S, Stripoli T, De Michele M, et al. ARDSnet ventilatory protocol and alveolar hyperinflation: role of positive end-expiratory pressure. American journal of respiratory and critical care medicine. 2007;176(8):761-767. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
