

Dual versus single vessel normothermic ex vivo perfusion of rat liver grafts using metamizole for vasodilatation
- PMID: 32614897
- PMCID: PMC7332079
- DOI: 10.1371/journal.pone.0235635
Dual versus single vessel normothermic ex vivo perfusion of rat liver grafts using metamizole for vasodilatation
Abstract
Background: Normothermic ex vivo liver perfusion (NEVLP) is a promising strategy to increase the donor pool in liver transplantation. Small animal models are essential to further investigate questions regarding organ preservation and reconditioning by NEVLP. A dual vessel small animal NEVLP (dNEVLP) model was developed using metamizole as a vasodilator and compared to conventional portovenous single vessel NEVLP (sNEVLP).
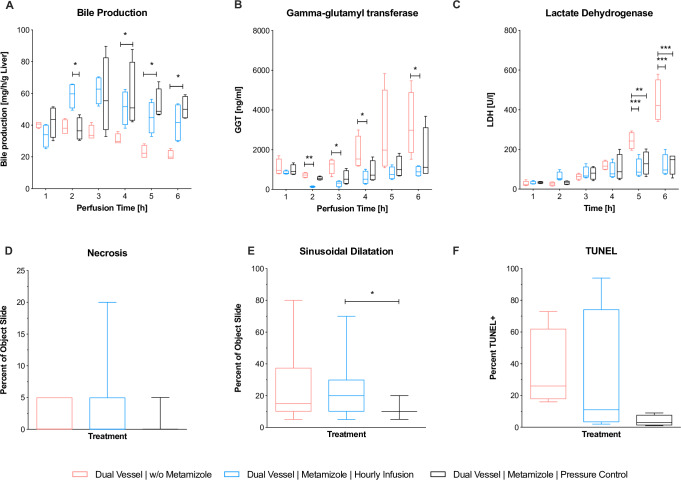
Methods: Livers of male Wistar rats were perfused with erythrocyte-supplemented culture medium for six hours by either dNEVLP via hepatic artery and portal vein or portovenous sNEVLP. dNEVLP was performed either with or without metamizole treatment. Perfusion pressure and flow rates were constantly monitored. Transaminase levels were determined in the perfusate at the start and after three and six hours of perfusion. Bile secretion was monitored and bile LDH and GGT levels were measured hourly. Histopathological analysis was performed using liver and bile duct tissue samples after perfusion.
Results: Hepatic artery pressure was significantly lower in dNEVLP with metamizole administration. Compared to sNEVLP, dNEVLP with metamizole treatment showed higher bile production, lower levels of transaminases during and after perfusion as well as significantly lower necrosis in liver and bile duct tissue. Biochemical markers of bile duct injury showed the same trend.
Conclusion: Our miniaturized dNEVLP system enables normothermic dual vessel rat liver perfusion. The administration of metamizole effectively ameliorates arterial vasospasm allowing for six hours of dNEVLP, with superior outcome compared to sNEVLP.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
