

High prevalence of non-communicable diseases among key populations enrolled at a large HIV prevention & treatment program in Kenya
- PMID: 32614906
- PMCID: PMC7332043
- DOI: 10.1371/journal.pone.0235606
High prevalence of non-communicable diseases among key populations enrolled at a large HIV prevention & treatment program in Kenya
Abstract
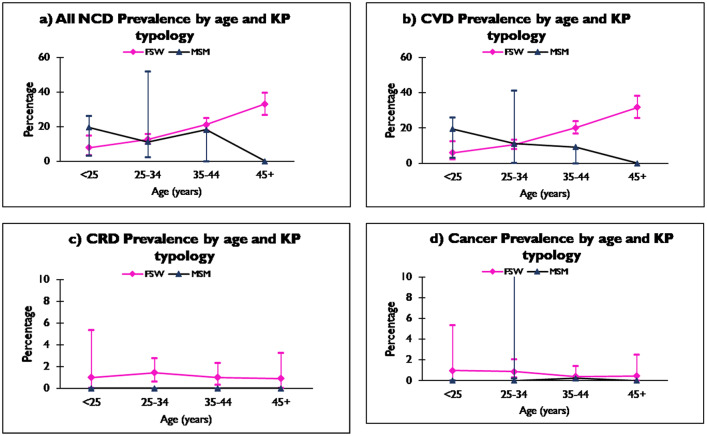
Introduction: People Living with HIV (PLHIV) bear a disproportionate burden of non-communicable diseases (NCDs). Despite their significant toll across populations globally, the NCD burden among key populations (KP) in Kenya remains unknown. The burden of four NCD-categories (cardiovascular diseases, cancer, chronic respiratory diseases and diabetes) was evaluated among female sex workers (FSWs) and men who have sex with men (MSM) at the Sex Workers Outreach Program (SWOP) clinics in Nairobi Kenya.
Methods: A retrospective medical chart review was conducted at the SWOP clinics among KP clients ≥15 years living with HIV enrolled between October 1, 2012 and September 30, 2015. The prevalence of the four NCD-categories were assessed at enrollment and during subsequent routine quarterly follow-up care visits as per the Ministry of Health guidelines. Prevalence at enrollment was determined and distributions of co-morbidities assessed using Chi-square and t-tests as appropriate during follow-up visits. Univariate and multivariate analysis were conducted to identify factors associated with NCD diagnoses.
Results: Overall, 1,478 individuals' records were analyzed; 1,392 (94.2%) were from FSWs while 86 (5.8%) were from MSM over the three-year period. FSWs' median age was 35.3 years (interquartile range (IQR) 30.1-41.6) while MSM were younger at 26.8 years (IQR 23.2-32.1). At enrollment into the HIV care program, most KPs (86.6%) were at an early WHO clinical stage (stage I-II) and 1462 (98.9%) were on first-line anti-retroviral therapy (ART). A total of 271, 18.3% (95% CI: 16.4-20.4%), KPs living with HIV had an NCD diagnosis in their clinical chart records during the study period. Majority of these cases, 258 (95.2%) were noted among FSWs. Cardiovascular disease that included hypertension was present in 249/271, 91.8%, of KPs with a documented NCD. Using a proxy of two or more elevated blood pressure readings taken < 12 months apart, prevalence of hypertension rose from 1.0% (95% CI: 0.6-1.7) that was documented in the charts during the first year to 16.3% (95% CI: 14.4-18.3) in the third year. Chronic respiratory disease mainly asthma was present in 16/271, a prevalence of 1.1% (95% CI: 0.6-1.8) in the study population. Cancer in general was detected in 10/271, prevalence of 0.7% (95% CI: 0.3-1.2) over the same period. Interestingly, diabetes was not noted in the study group. Lastly, significant associations between NCD diagnosis with increasing age, body-mass index and CD4 + cell-counts were noted in univariate analysis. However, except for categories of ≥ BMI 30 kg/m2 and age ≥ 45, the associations were not sustained in adjusted risk estimates.
Conclusion: In Kenya, KP living with HIV and on ART have a high prevalence of NCD diagnoses. Multiple NCD risk factors were also noted against a backdrop of a changing HIV epidemic in the study population. This calls for scaling up focus on both HIV and NCD prevention and care in targeted populations at increased risk of HIV acquisition and transmission. Hence, KP programs could include integrated HIV-NCD screening and care in their guidelines.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kyu HH, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018;392(10159):1859–922. Epub 2018/11/13. 10.1016/s0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- WHO. A heavy burden: the productivity cost of illness in Africa Brazzaville, Congo: WHO Regional Office for Africa; 2019. https://www.afro.who.int/publications/heavy-burden-productivity-cost-ill....
-
- Kirigia J, Mwabu G. The Indirect cost of illness in Africa2018.
-
- Patel P, Rose CE, Collins PY, Nuche-Berenguer B, Sahasrabuddhe VV, Peprah E, et al. Noncommunicable diseases among HIV-infected persons in low-income and middle-income countries: a systematic review and meta-analysis. Aids. 2018;32 Suppl 1:S5–s20. Epub 2018/06/29. 10.1097/qad.0000000000001888 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
