

DLBCL patients treated with CD19 CAR T cells experience a high burden of organ toxicities but low nonrelapse mortality
- PMID: 32614964
- PMCID: PMC7362382
- DOI: 10.1182/bloodadvances.2020001972
DLBCL patients treated with CD19 CAR T cells experience a high burden of organ toxicities but low nonrelapse mortality
Abstract
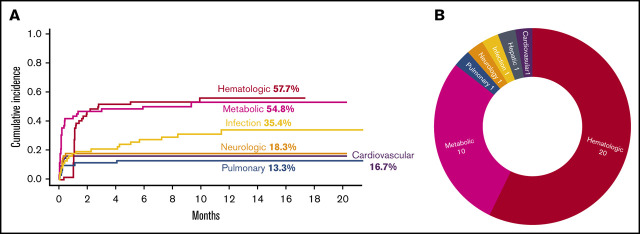
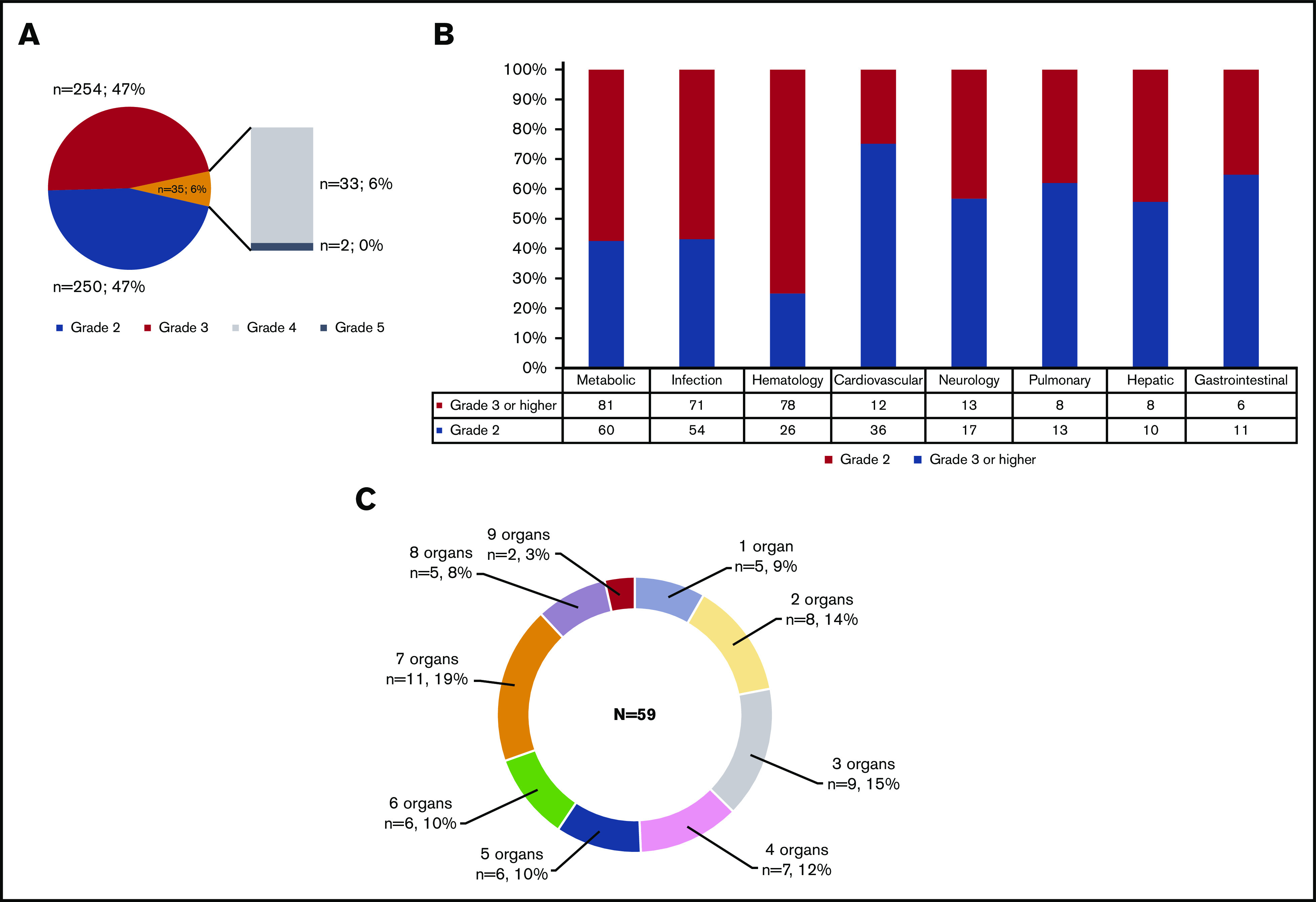
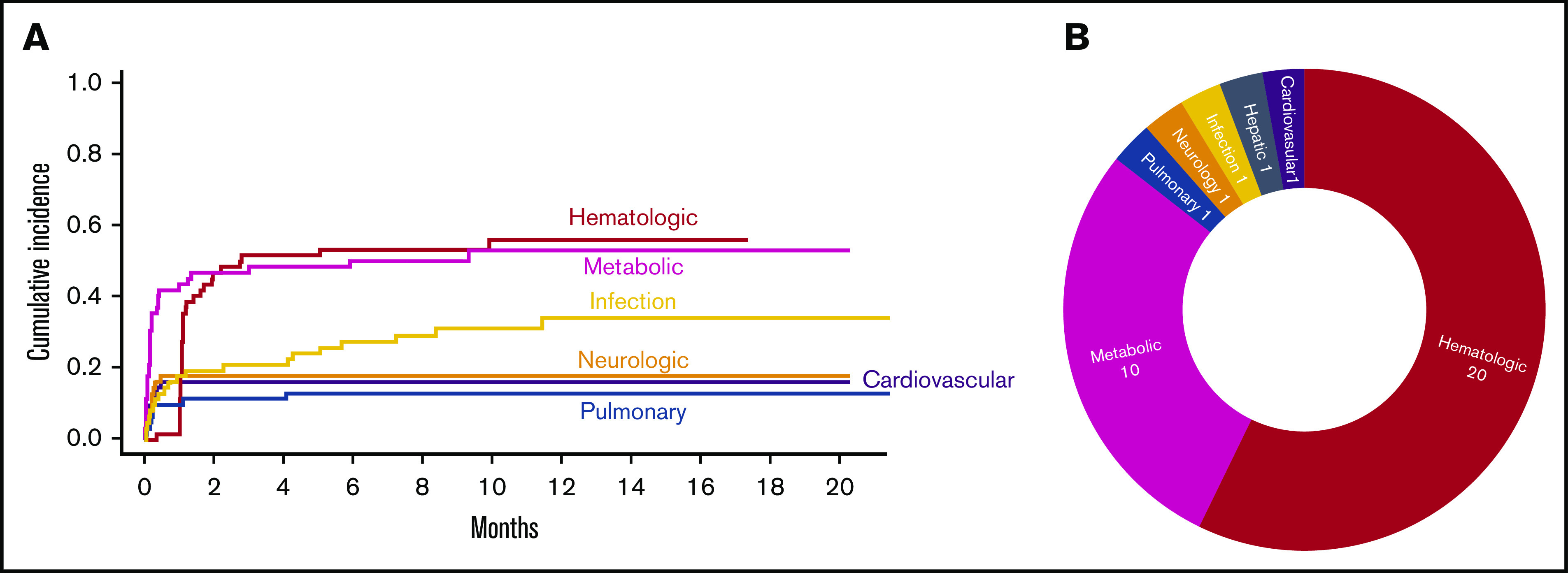
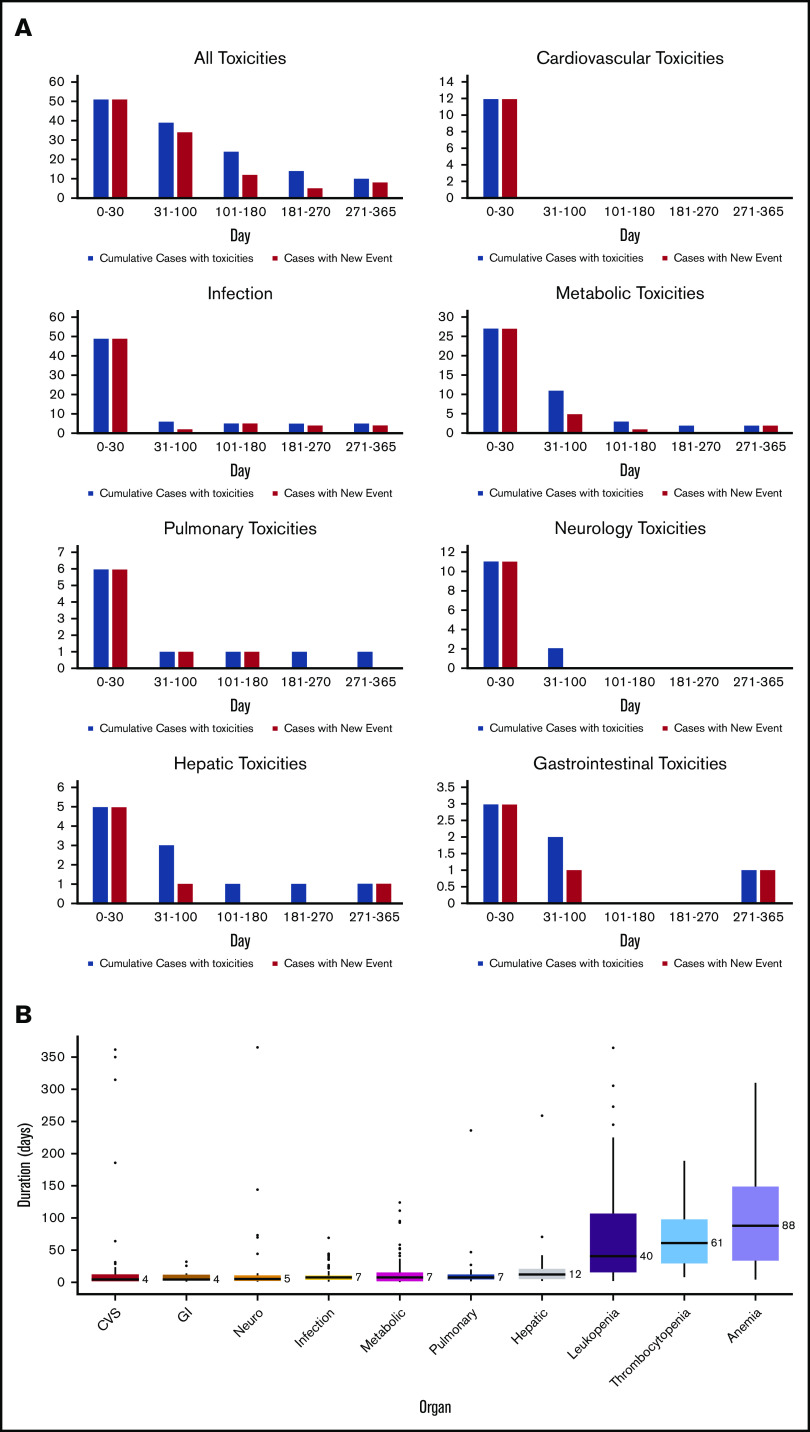
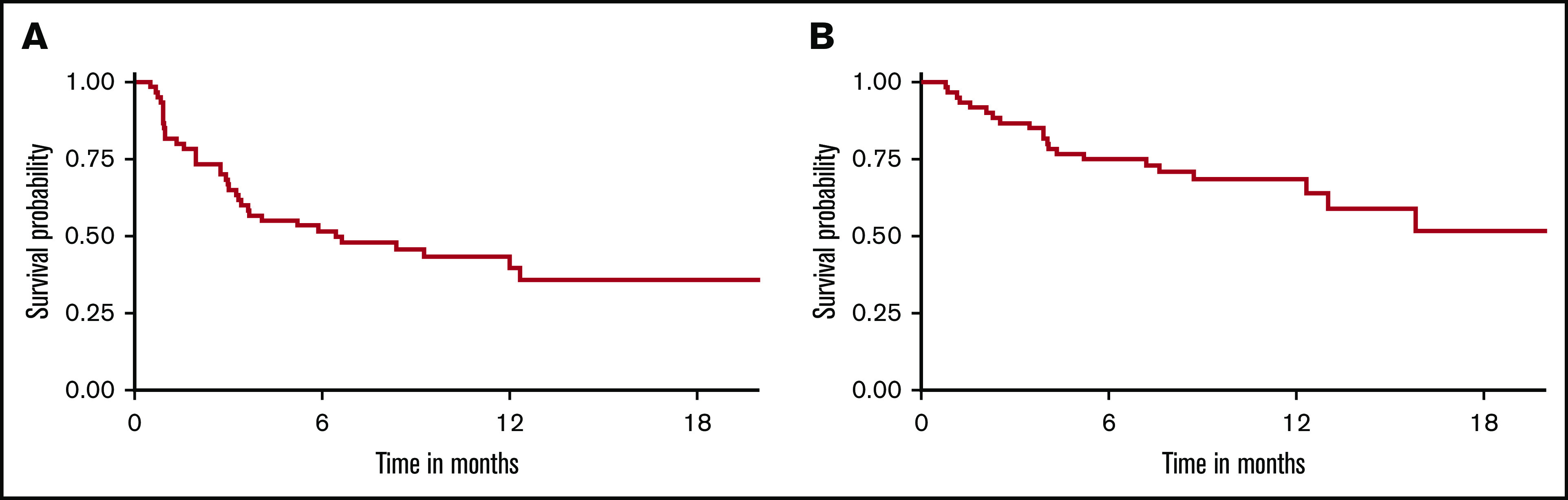
Cytokine release syndrome (CRS) immune effector cell-associated neurotoxicity syndrome are the most notable toxicities of CD19 chimeric antigen receptor (CAR) T-cell therapy. In addition, CAR T-cell-mediated toxicities can involve any organ system, with varied impacts on outcomes, depending on patient factors and involved organs. We performed detailed analysis of organ-specific toxicities and their association with outcomes in 60 patients with diffuse large B-cell lymphoma (DLBCL) treated with CD19 CAR T cells by assessing all toxicities in organ-based groups during the first year posttreatment. We observed 539 grade ≥2 and 289 grade ≥3 toxicities. Common grade ≥3 toxicities included hematological, metabolic, infectious, and neurological complications, with corresponding 1-year cumulative incidence of 57.7%, 54.8%, 35.4%, and 18.3%, respectively. Patients with impaired performance status had a higher risk of grade ≥3 metabolic complications, whereas elevated lactate dehydrogenase was associated with higher risks of grade ≥3 neurological and pulmonary toxicities. CRS was associated with higher incidence of grade ≥3 metabolic, pulmonary, and neurologic complications. The 1-year nonrelapse mortality and overall survival were 1.7% and 69%, respectively. Only grade ≥3 pulmonary toxicities were associated with an increased mortality risk. In summary, toxicity burdens after CD19 CAR T-cell therapy were high and varied by organ systems. Most toxicities were manageable and were rarely associated with mortality. Our study emphasizes the importance of toxicity assessment, which could serve as a benchmark for further research to reduce symptom burdens and improve tolerability in patients treated with CAR T cells.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: K.W. receives salary support from Parker Institute for Cancer Immunotherapy at Memorial Sloan Kettering Cancer Center. M.P. received salary support from an American Italian Cancer Foundation Postdoctoral Research Fellowship and from Associazione Italiana contro le Leucemie-linfomi e mieloma Milano e Provincia Organizzazione Non Lucrativa di Utilità Sociale. M.G.-R. reports receiving honoraria from Takeda and Janssen Pharmaceutical. M.S. has served as a paid consultant for McKinsey & Company, Angiocrine Bioscience, Inc, and Omeros Corporation; has received research funding from Angiocrine Bioscience, Inc; and has served on an ad hoc advisory board for Kite, a Gilead Company. G.L.S. receives research funding from Amgen and Janssen Pharmaceutical. C.L.B. serves as a paid consultant for Life Sci, GLG, Juno/Celgene, Seattle Genetics, and Kite/Gilead; reports receiving research funding from Janssen Pharmaceutical, Novarits, Epizume, Xynomics, and Bayer; and receives honorarium from Dava Oncology. M.L.P. has served on ad hoc advisory boards for Kite and Novartis. P.B.D. serves on the advisory board for Kite/Gilead. C.S.S. has served as a paid consultant on advisory boards for Juno Therapeutics, Sanofi-Genzyme, Spectrum Pharmaceuticals, Novartis, Genmab, Precision Biosciences, Kite, a Gilead Company, Celgene, Gamida Cell, and GlaxoSmithKline; and has received research funds for clinical trials from Juno Therapeutics, Celgene, Precision Biosciences, and Sanofi-Genzyme. B.D.S. provides consultancy for Kite/Gilead, Juno/Celgene, and Janssen; and also receives research support from ADC Therapeutics. M.-A.P. reports honoraria from Kite/Gilead, AbbVie, Bellicum, Bristol-Myers Squibb, Incyte, Merck, Novartis, Nektar Therapeutics, Omeros, and Takeda; serves on data and safety monitoring boards for Servier and Medigene, and the scientific advisory boards of MolMed and NexImmune; has received research support for clinical trials from Incyte, Kite/Gilead, and Miltenyi Biotec; and serves in a volunteer capacity as a member of the Board of Directors of the American Society for Transplantation and Cellular Therapy (ASTCT) and Be the Match (National Marrow Donor Program [NMDP]), as well as on the Center for International Blood & Marrow Transplant Research (CIBMTR) Cellular Immunotherapy Data Resource (CIDR) Committee. The remaining authors declare no competing financial interests.
Figures
References
-
- Santomasso B, Bachier C, Westin J, Rezvani K, Shpall EJ. The other side of CAR T-cell therapy: cytokine release syndrome, neurologic toxicity, and financial burden. Am Soc Clin Oncol Educ Book. 2019;39(39):433-444. - PubMed
-
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs.... Accessed 7 February 2020.
