

Complicated hospitalization due to influenza: results from the Global Hospital Influenza Network for the 2017-2018 season
- PMID: 32615985
- PMCID: PMC7330273
- DOI: 10.1186/s12879-020-05167-4
Complicated hospitalization due to influenza: results from the Global Hospital Influenza Network for the 2017-2018 season
Abstract
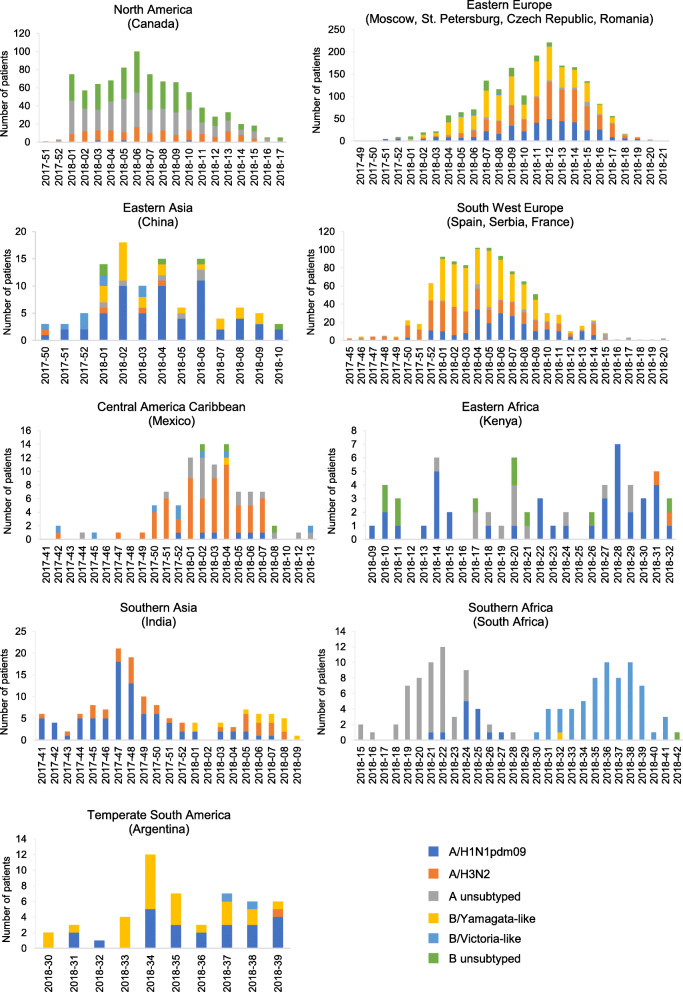
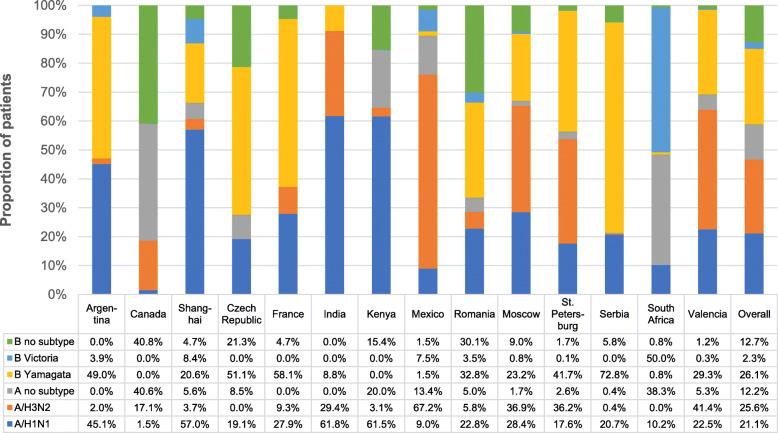
Background: Since 2011, the Global Influenza Hospital Surveillance Network (GIHSN) has used active surveillance to prospectively collect epidemiological and virological data on patients hospitalized with influenza virus infection. Here, we describe influenza virus strain circulation in the GIHSN participant countries during 2017-2018 season and examine factors associated with complicated hospitalization among patients admitted with laboratory-confirmed influenza illness.
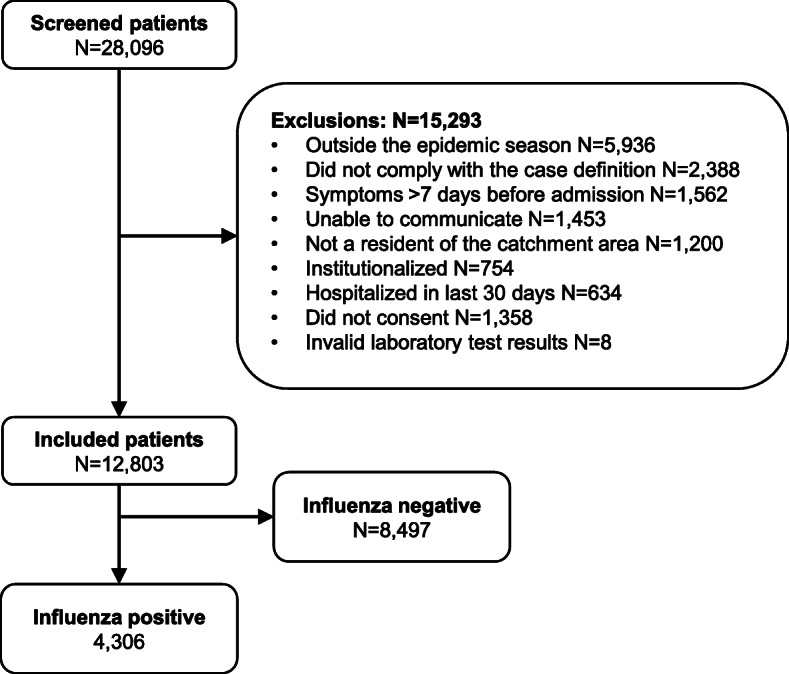
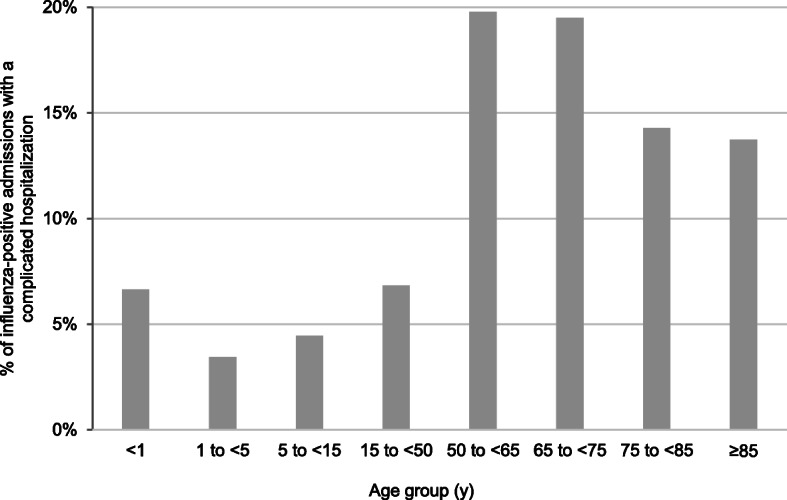
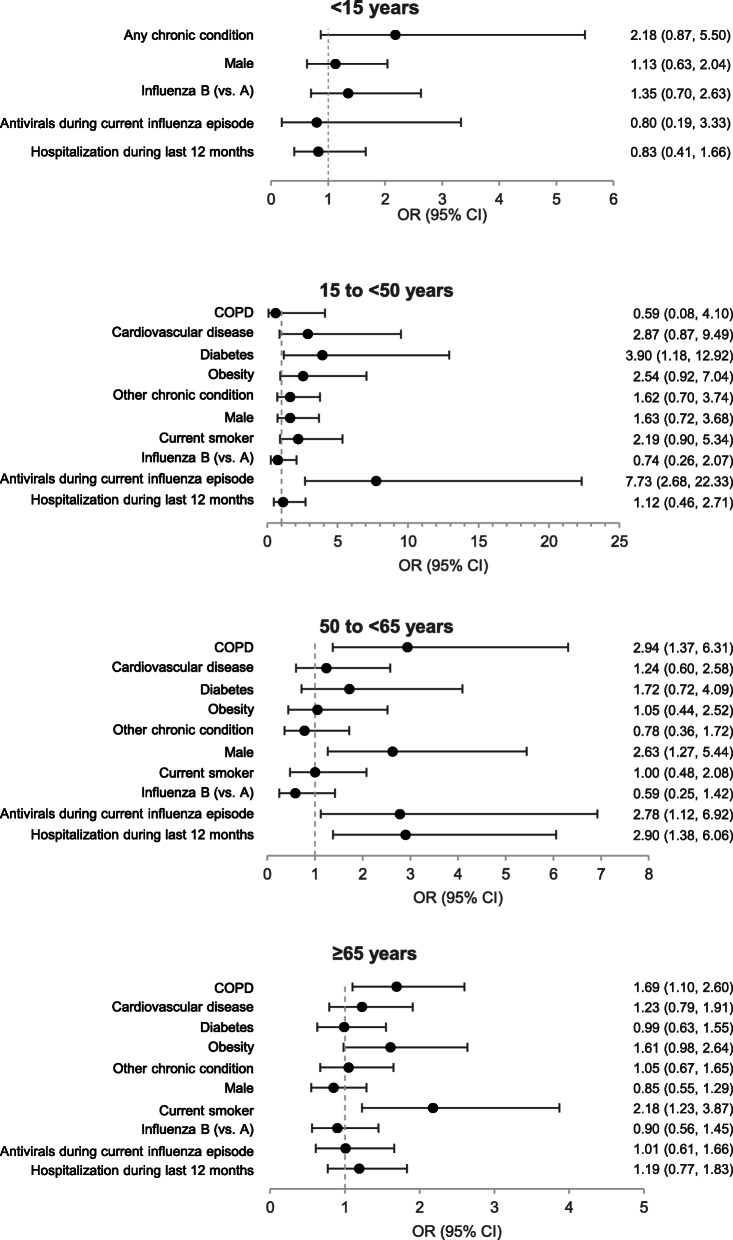
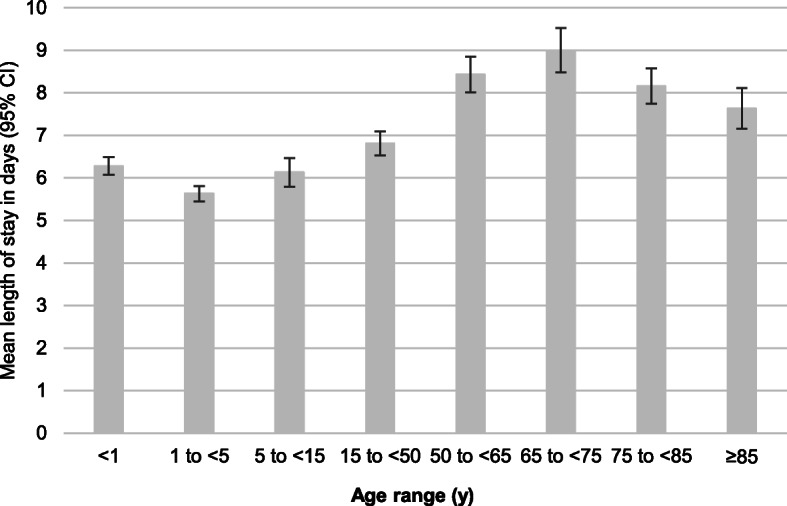
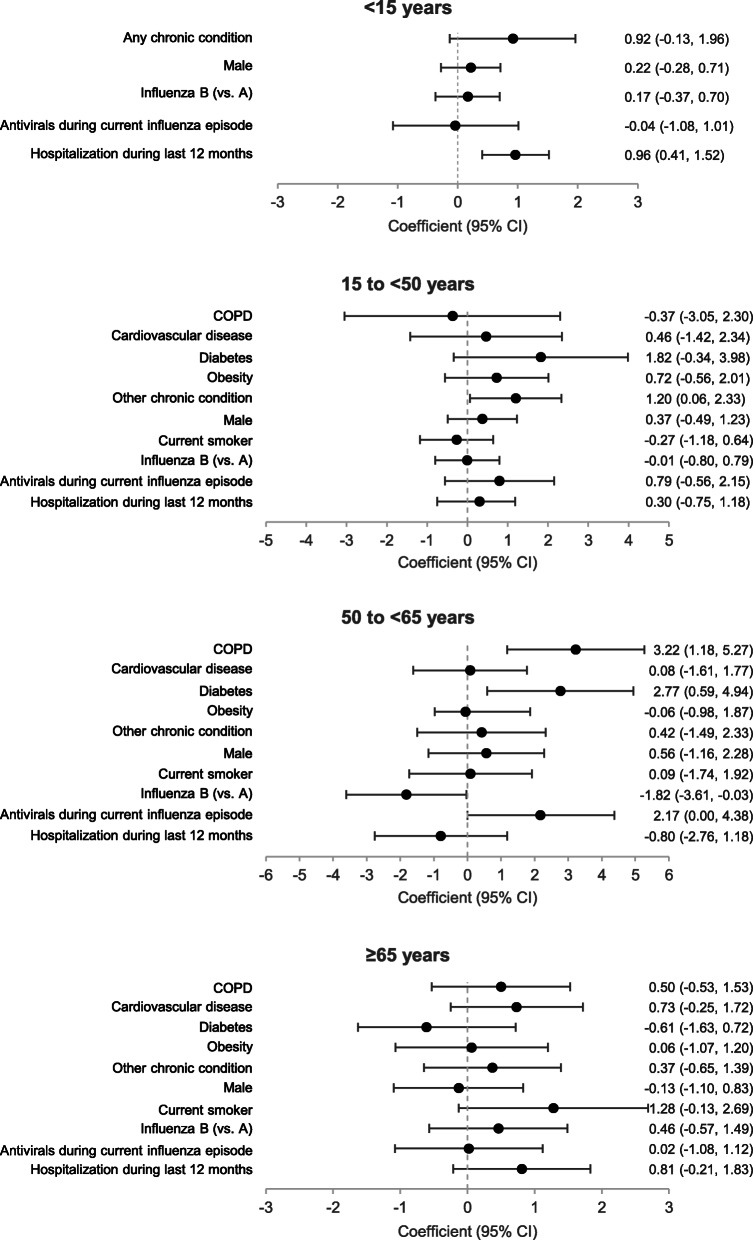
Methods: The study enrolled patients who were hospitalized in a GIHSN hospital in the previous 48 h with acute respiratory symptoms and who had symptoms consistent with influenza within the 7 days before admission. Enrolled patients were tested by reverse transcription-polymerase chain reaction to confirm influenza virus infection. "Complicated hospitalization" was defined as a need for mechanical ventilation, admission to an intensive care unit, or in-hospital death. In each of four age strata (< 15, 15-< 50, 50-< 65, and ≥ 65 years), factors associated with complicated hospitalization in influenza-positive patients were identified by mixed effects logistic regression and those associated with length of hospital stay using a linear mixed-effects regression model.
Results: The study included 12,803 hospitalized patients at 14 coordinating sites in 13 countries, of which 4306 (34%) tested positive for influenza. Influenza viruses B/Yamagata, A/H3N2, and A/H1N1pdm09 strains dominated and cocirculated, although the dominant strains varied between sites. Complicated hospitalization occurred in 10.6% of influenza-positive patients. Factors associated with complicated hospitalization in influenza-positive patients included chronic obstructive pulmonary disease (15-< 50 years and ≥ 65 years), diabetes (15-< 50 years), male sex (50-< 65 years), hospitalization during the last 12 months (50-< 65 years), and current smoking (≥65 years). Chronic obstructive pulmonary disease (50-< 65 years), other chronic conditions (15-< 50 years), influenza A (50-< 65 years), and hospitalization during the last 12 months (< 15 years) were associated with a longer hospital stay. The proportion of patients with complicated influenza did not differ between influenza A and B.
Conclusions: Complicated hospitalizations occurred in over 10% of patients hospitalized with influenza virus infection. Factors commonly associated with complicated or longer hospitalization differed by age group but commonly included chronic obstructive pulmonary disease, diabetes, and hospitalization during the last 12 months.
Keywords: Epidemiology; Hospitalization; Influenza; Mortality; Risk factors.
Conflict of interest statement
J.P. received research funds from the Foundation for Influenza Epidemiology for work related to this study and unrestricted research grants for work unrelated to the current study from Sanofi Pasteur (which provides financial support for the Foundation for Influenza Epidemiology). P.V. and M.N. received research funds from the Foundation for Influenza Epidemiology for work related to this study and personal fees from Sanofi Pasteur for work unrelated to the current study. M.K.A. and S.A.M. received research funds from the Foundation for Influenza Epidemiology for work related to this study and grants and personal fees from Sanofi Pasteur for work unrelated to the current study. J.K. received research funds from the Foundation for Influenza Epidemiology for work related to this study. A.G. was an employee of OpenHealth, which is paid by the Foundation for Influenza Epidemiology for work related to this study. All other authors declare no conflicts of interest.
Figures
References
-
- World Health Organization: Influenza (Seasonal). https://www.who.int/en/news-room/fact-sheets/detail/influenza-(seasonal) . Accessed 02 Jul 2019. (2012).
-
- World Health Organization Vaccines against influenza WHO position paper - November 2012. Wkly Epidemiol Rec. 2012;87:461–476. - PubMed
-
- Coleman BL, Fadel SA, Fitzpatrick T, Thomas SM. Risk factors for serious outcomes associated with influenza illness in high- versus low- and middle-income countries: systematic literature review and meta-analysis. Influenza Other Respir Viruses. 2018;12:22–29. doi: 10.1111/irv.12504. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
