

Histopathological findings for prediction of liver cirrhosis and survival in biliary atresia patients after Kasai procedure
- PMID: 32616059
- PMCID: PMC7333324
- DOI: 10.1186/s13000-020-00996-y
Histopathological findings for prediction of liver cirrhosis and survival in biliary atresia patients after Kasai procedure
Abstract
Background: Without early recognition and Kasai procedure, biliary atresia (BA) results in liver cirrhosis and leads to either transplantation or death at a young age. We aimed to characterize the liver histopathological findings for prediction of cirrhosis and survival in BA patients after Kasai surgery.
Methods: We retrospectively reviewed all histopathological results for BA patients who underwent liver biopsy during Kasai surgery from August 2012 to December 2018 in Dr. Sardjito Hospital, Yogyakarta, Indonesia.
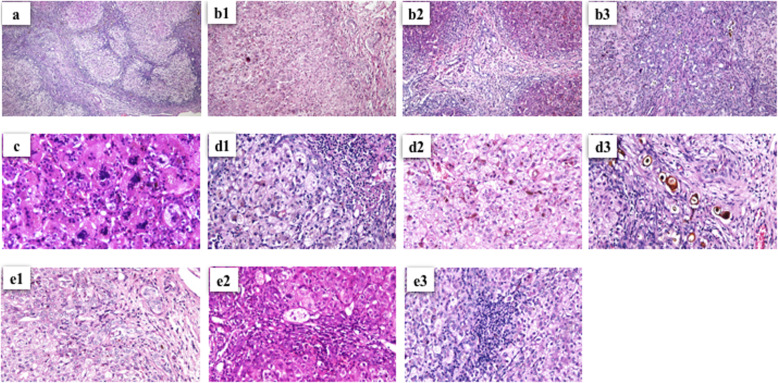
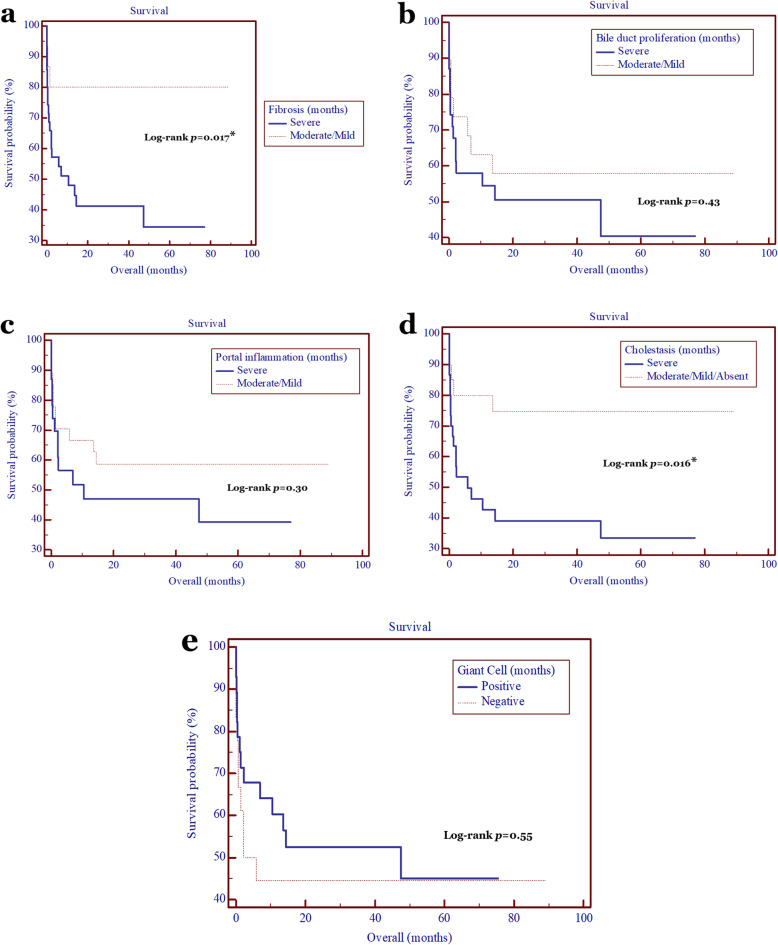
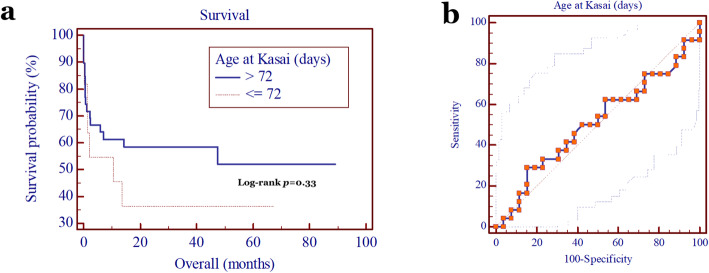
Results: Fifty infants with BA were ascertained in our study, of whom 27 were males and 23 were females. The median age of Kasai procedure was 102.5 days (interquartile range (IQR), 75.75-142.25 days). There were 33 (66%) and 17 (34%) BA patients with and without liver cirrhosis, respectively, while the overall survival was 52%. The patients with a severe bile duct proliferation, severe cholestasis, and severe portal inflammation have a higher risk by 27-, 22-, and 19.3-fold, respectively, to develop liver cirrhosis compared with patients with a moderate/mild bile duct proliferation, moderate/mild/without cholestasis, and moderate/mild portal inflammation, respectively (p = 3.6 × 10- 6, 5.6 × 10- 4, and 1.6 × 10- 3, respectively), while the giant cell transformation was not associate with the development of liver cirrhosis (p = 0.77). The bile duct proliferation was strongly correlated with cholestasis and portal inflammation (p = 7.3 × 10- 5 and 2 × 10- 4, respectively), and cholestasis was also significantly correlated with portal inflammation (p = 0.016). Interestingly, the age at Kasai procedure was strongly associated with the development of liver cirrhosis (p = 0.02), but not with the patients' survival (p = 0.33), while the degree of fibrosis and cholestasis were significantly correlated with the patients' survival, with HR of 3.9 (95% CI = 1.7-9.0; p = 0.017) and 3.1 (95% CI = 1.4-7.0; p = 0.016), respectively.
Conclusions: Histopathological findings of bile duct proliferation, cholestasis, and portal inflammation can predict the liver cirrhosis development in patients with BA. Furthermore, degree of fibrosis and cholestasis affect the patients' survival following the Kasai operation.
Keywords: Biliary atresia; Histopathological findings; Kasai procedure; Liver cirrhosis; Patient survival; Prognosis.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
