

Systemic therapy for advanced clear cell renal cell carcinoma after discontinuation of immune-oncology and VEGF targeted therapy combinations
- PMID: 32616076
- PMCID: PMC7331268
- DOI: 10.1186/s12894-020-00647-w
Systemic therapy for advanced clear cell renal cell carcinoma after discontinuation of immune-oncology and VEGF targeted therapy combinations
Abstract
Background: Several phase 3 studies reported positive results for combinations of Immune-Oncology (IO) and Vascular Endothelial Growth Factor (VEGF) targeted therapies in patients with metastatic clear cell Renal Cell Carcinoma (ccRCC). However, there are limited data on outcomes to systemic therapy after IO-VEGF combinations.
Methods: A retrospective analysis was performed on patients with metastatic ccRCC treated at the Memorial Sloan Kettering Cancer Center and Cleveland Clinic who initiated systemic therapy post IO-VEGF including combinations with VEGF receptor (VEGFR) tyrosine kinase inhibitors (IO-TKI) and combinations with the anti-VEGF monoclonal antibody bevacizumab (IO-Bev). The study objectives were to evaluate the objective response rate (ORR), progression-free survival (PFS) and overall survival (OS) on systemic therapy post IO-VEGF. RECIST v1.1 criteria were used to determine radiological responses and progression. Survival estimates were evaluated with the Kaplan-Meier methods and the log-rank test from the start of systemic therapy post IO-VEGF to the event of interest.
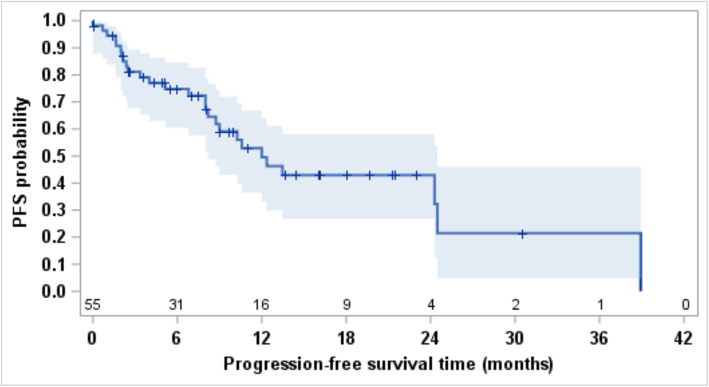
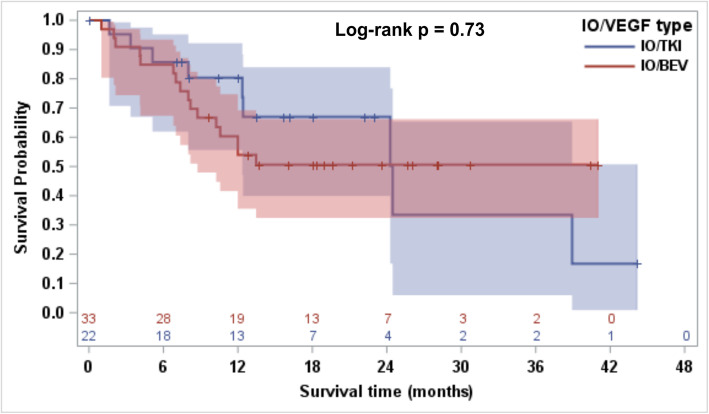
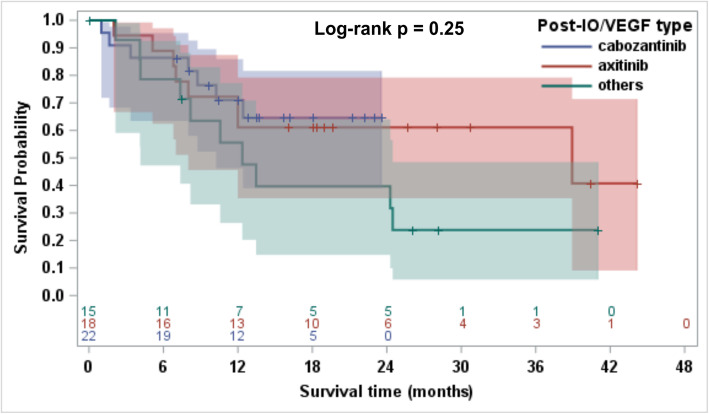
Results: A total of fifty-nine patients were treated post discontinuation of IO-VEGF regimens which included IO-Bev (n = 35; 59%) and IO-TKI (n = 24; 41%). Fifty-eight patients (98%) received IO-VEGF regimens as part of a clinical trial. Subsequent therapies included cabozantinib (n = 22; 37%), axitinib (n = 18; 31%), pazopanib (n = 4; 7%), lenvatinib and everolimus (n = 4; 7%), mTOR inhibitor monotherapy (n = 3; 5%), axitinib and dalantercept (n = 2; 3%), sunitinib (n = 1; 2%), sorafenib (n = 1; 2%), and treatment with agents on unreported clinical trials (n = 4; 7%). Patients treated on unreported clinical trials were excluded from the efficacy analysis. Post IO-VEGF, the ORR was 25% and median PFS was 12.0 months (95% CI, 8.2-24.5). Median OS was 24.5 months (95% CI, 12-NE) and 12 months OS rate was 63.3% (95% CI, 48.6-74.9). We observed no differences post IO-VEGF OS when comparing IO- TKI vs IO-Bev (Log-rank p = 0.73).
Conclusions: Post IO-VEGF, most patients received VEGFR-TKIs. In this setting, VEGFR-TKIs demonstrated clinical activity and remain a viable option for salvage therapy after progression on IO-VEGF.
Keywords: IO combinations; Immune-oncology; RCC; Survival; VEGF.
Conflict of interest statement
Yasser Ged has no relationships to disclose.
Ruby Gupta has no relationships to disclose.
Cihan Duzgol has no relationships to disclose.
Andrea Knezevic has no relationships to disclose.
Natalie Shapnik has no relationships to disclose.
Ritesh Kotecha has no relationships to disclose.
Martin H. Voss reports receiving commercial research grants from Bristol-Myers Squibb and Genentech/Roche. Honoraria from Novartis. Travel/accommodation from Eisai, Novartis, and Takeda. Consultant/advisory board member for- Alexion Pharmaceuticals, Bayer, Calithera Biosciences, Corvus Pharmaceuticals, Exelixis, Eisai, GlaxoSmithKline, Natera, Novartis, and Pfizer.
Darren R. Feldman reports research support from Novartis and Seattle Genetics.
Oguz Akin has no relationships to disclose.
Sujata Patil has no relationships to disclose.
Robert J. Motzer reports receiving commercial research grants from Pfizer, Eisai, Exelixis, Bristol-Myers Squibb, Genentech/Roche, and Novartis, and is a consultant/advisory board member for Pfizer, Merck, Genentech, Exelixis, Eisai, and Novartis.
Brian Rini reports receiving research funding from Pfizer, Merck, GNE/Roche, Peloton, Aveo, Astra-Zeneca, and BMS, and is consultant/advisory board member for BMS, Pfizer, Aveo, GNE/Roche, Compugen, Merck, Corvus, and Exelixis, and holds stocks in PTC Therapeutics.
Chung-Han Lee reports receiving commercial research grants from BMS, Eisai, Exelixis, Pfizer, and Calithera, and is a consultant/advisory board member for Amgen, BMS, Exelixis, and Eisai.
Figures

Similar articles
-
Lenvatinib with or Without Everolimus in Patients with Metastatic Renal Cell Carcinoma After Immune Checkpoint Inhibitors and Vascular Endothelial Growth Factor Receptor-Tyrosine Kinase Inhibitor Therapies.Oncologist. 2021 Jun;26(6):476-482. doi: 10.1002/onco.13770. Epub 2021 Apr 21. Oncologist. 2021. PMID: 33792094 Free PMC article.
-
Real-world Outcome of Patients with Advanced Renal Cell Carcinoma and Intermediate- or Poor-risk International Metastatic Renal Cell Carcinoma Database Consortium Criteria Treated by Immune-oncology Combinations: Differential Effectiveness by Risk Group?Eur Urol Oncol. 2024 Feb;7(1):102-111. doi: 10.1016/j.euo.2023.07.003. Epub 2023 Jul 21. Eur Urol Oncol. 2024. PMID: 37481365
-
Combination antiangiogenic tyrosine kinase inhibition and anti-PD1 immunotherapy in metastatic renal cell carcinoma: A retrospective analysis of safety, tolerance, and clinical outcomes.Cancer Med. 2021 Apr;10(7):2341-2349. doi: 10.1002/cam4.3812. Epub 2021 Mar 1. Cancer Med. 2021. PMID: 33650321 Free PMC article.
-
Optimal management of metastatic renal cell carcinoma: current status.Drugs. 2013 Apr;73(5):427-38. doi: 10.1007/s40265-013-0043-1. Drugs. 2013. PMID: 23572408 Review.
-
Systemic therapy in metastatic renal cell carcinoma.World J Urol. 2017 Feb;35(2):179-188. doi: 10.1007/s00345-016-1868-5. Epub 2016 Jun 9. World J Urol. 2017. PMID: 27277600 Free PMC article. Review.
Cited by
-
An Overview of Systemic Targeted Therapy in Renal Cell Carcinoma, with a Focus on Metastatic Renal Cell Carcinoma and Brain Metastases.Curr Issues Mol Biol. 2023 Sep 21;45(9):7680-7704. doi: 10.3390/cimb45090485. Curr Issues Mol Biol. 2023. PMID: 37754269 Free PMC article. Review.
-
Subgroup analysis of the AFTER I-O study: a retrospective study on the efficacy and safety of subsequent molecular targeted therapy after immune-oncology therapy in Japanese patients with metastatic renal cell carcinoma.Jpn J Clin Oncol. 2021 Nov 1;51(11):1656-1664. doi: 10.1093/jjco/hyab114. Jpn J Clin Oncol. 2021. PMID: 34350454 Free PMC article.
-
Cell Differentiation Trajectory Predicts Prognosis and Immunotherapeutic Response in Clear Cell Renal Cell Carcinoma.Genet Res (Camb). 2022 Nov 29;2022:8422339. doi: 10.1155/2022/8422339. eCollection 2022. Genet Res (Camb). 2022. PMID: 36530957 Free PMC article.
-
Antiangiogenic Properties of Axitinib versus Sorafenib Following Sunitinib Resistance in Human Endothelial Cells-A View towards Second Line Renal Cell Carcinoma Treatment.Biomedicines. 2021 Nov 6;9(11):1630. doi: 10.3390/biomedicines9111630. Biomedicines. 2021. PMID: 34829859 Free PMC article.
-
Lenvatinib with or Without Everolimus in Patients with Metastatic Renal Cell Carcinoma After Immune Checkpoint Inhibitors and Vascular Endothelial Growth Factor Receptor-Tyrosine Kinase Inhibitor Therapies.Oncologist. 2021 Jun;26(6):476-482. doi: 10.1002/onco.13770. Epub 2021 Apr 21. Oncologist. 2021. PMID: 33792094 Free PMC article.
References
-
- Selby MJ, Engelhardt JJ, Johnston RJ, Lu LS, Han M, Thudium K, et al. Preclinical development of Ipilimumab and Nivolumab combination immunotherapy: mouse tumor models, in vitro functional studies, and cynomolgus macaque toxicology. PLoS One. 2016;11(9):e0161779. doi: 10.1371/journal.pone.0161779. - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
