

Accuracy of identifying incident stroke cases from linked health care data in UK Biobank
- PMID: 32616677
- PMCID: PMC7455356
- DOI: 10.1212/WNL.0000000000009924
Accuracy of identifying incident stroke cases from linked health care data in UK Biobank
Abstract
Objective: In UK Biobank (UKB), a large population-based prospective study, cases of many diseases are ascertained through linkage to routinely collected, coded national health datasets. We assessed the accuracy of these for identifying incident strokes.
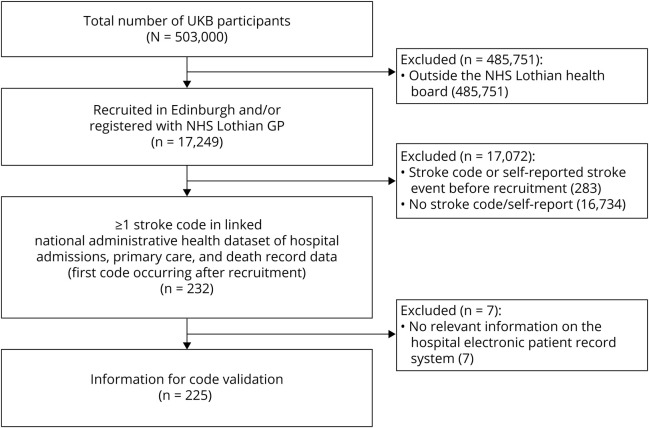
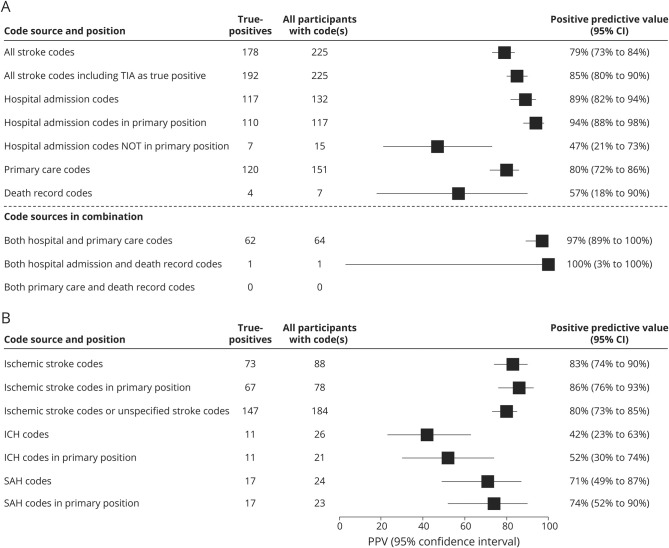
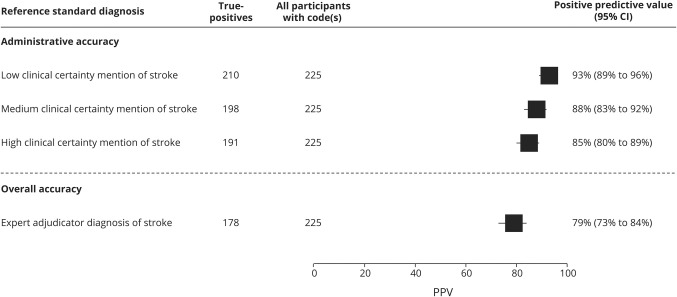
Methods: In a regional UKB subpopulation (n = 17,249), we identified all participants with ≥1 code signifying a first stroke after recruitment (incident stroke-coded cases) in linked hospital admission, primary care, or death record data. Stroke physicians reviewed their full electronic patient records (EPRs) and generated reference standard diagnoses. We evaluated the number and proportion of cases that were true-positives (i.e., positive predictive value [PPV]) for all codes combined and by code source and type.
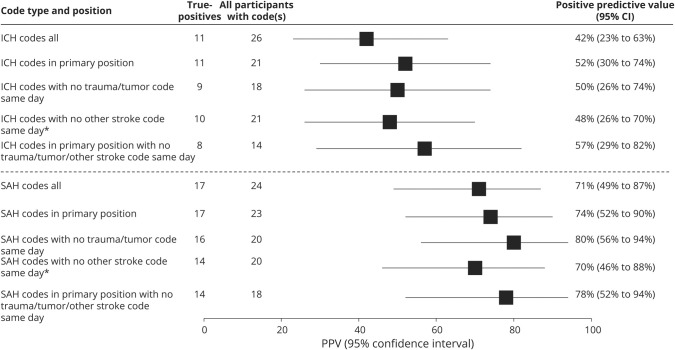
Results: Of 232 incident stroke-coded cases, 97% had EPR information available. Data sources were 30% hospital admission only, 39% primary care only, 28% hospital and primary care, and 3% death records only. While 42% of cases were coded as unspecified stroke type, review of EPRs enabled a pathologic type to be assigned in >99%. PPVs (95% confidence intervals) were 79% (73%-84%) for any stroke (89% for hospital admission codes, 80% for primary care codes) and 83% (74%-90%) for ischemic stroke. PPVs for small numbers of death record and hemorrhagic stroke codes were low but imprecise.
Conclusions: Stroke and ischemic stroke cases in UKB can be ascertained through linked health datasets with sufficient accuracy for many research studies. Further work is needed to understand the accuracy of death record and hemorrhagic stroke codes and to develop scalable approaches for better identifying stroke types.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Comment: Can we trust administrative codes for identification of stroke cases?Neurology. 2020 Aug 11;95(6):250. doi: 10.1212/WNL.0000000000009931. Epub 2020 Jul 2. Neurology. 2020. PMID: 32616676 No abstract available.
References
-
- Woodfield R, Grant I, UK Biobank Stroke Outcomes Group, UK Biobank Follow-Up and Outcomes Working Group, Sudlow CL. Accuracy of electronic health record data for identifying stroke cases in large-scale epidemiological studies: a systematic review from the UK Biobank stroke outcomes group. PLoS One 2015;10:e0140533. - PMC - PubMed
-
- WHO MONICA Project Investigators. The World Health Organization MONICA project (Monitoring Trends and Determinants in Cardiovascular Disease). J Clin Epidemiol 1988;41:105–114. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous