

Pediatric Distraction on Induction of Anesthesia With Virtual Reality and Perioperative Anxiolysis: A Randomized Controlled Trial
- PMID: 32618627
- PMCID: PMC9387568
- DOI: 10.1213/ANE.0000000000005004
Pediatric Distraction on Induction of Anesthesia With Virtual Reality and Perioperative Anxiolysis: A Randomized Controlled Trial
Abstract
Background: Perioperative pediatric anxiety is common and can have a negative psychological impact on children undergoing surgery and anesthesia. Studies have shown an incidence of anxiety at induction of up to 50%. Audiovisual distraction, including virtual reality (VR), is a noninvasive, nonpharmacological modality that may reduce perioperative anxiety. The goal of this study was to determine whether immersive audiovisual distraction with a VR headset during induction of general anesthesia (GA) in pediatric patients reduced preoperative anxiety.
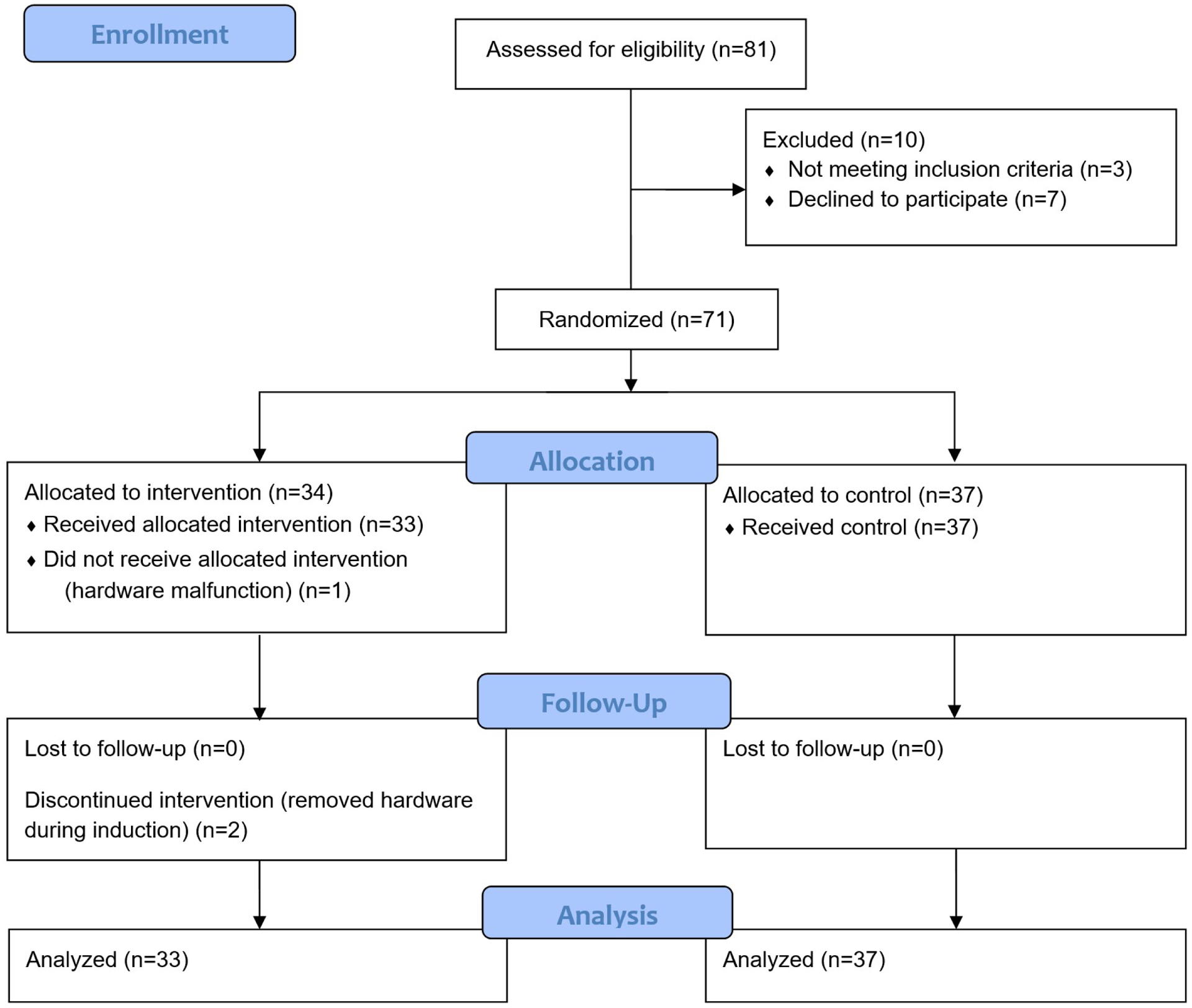
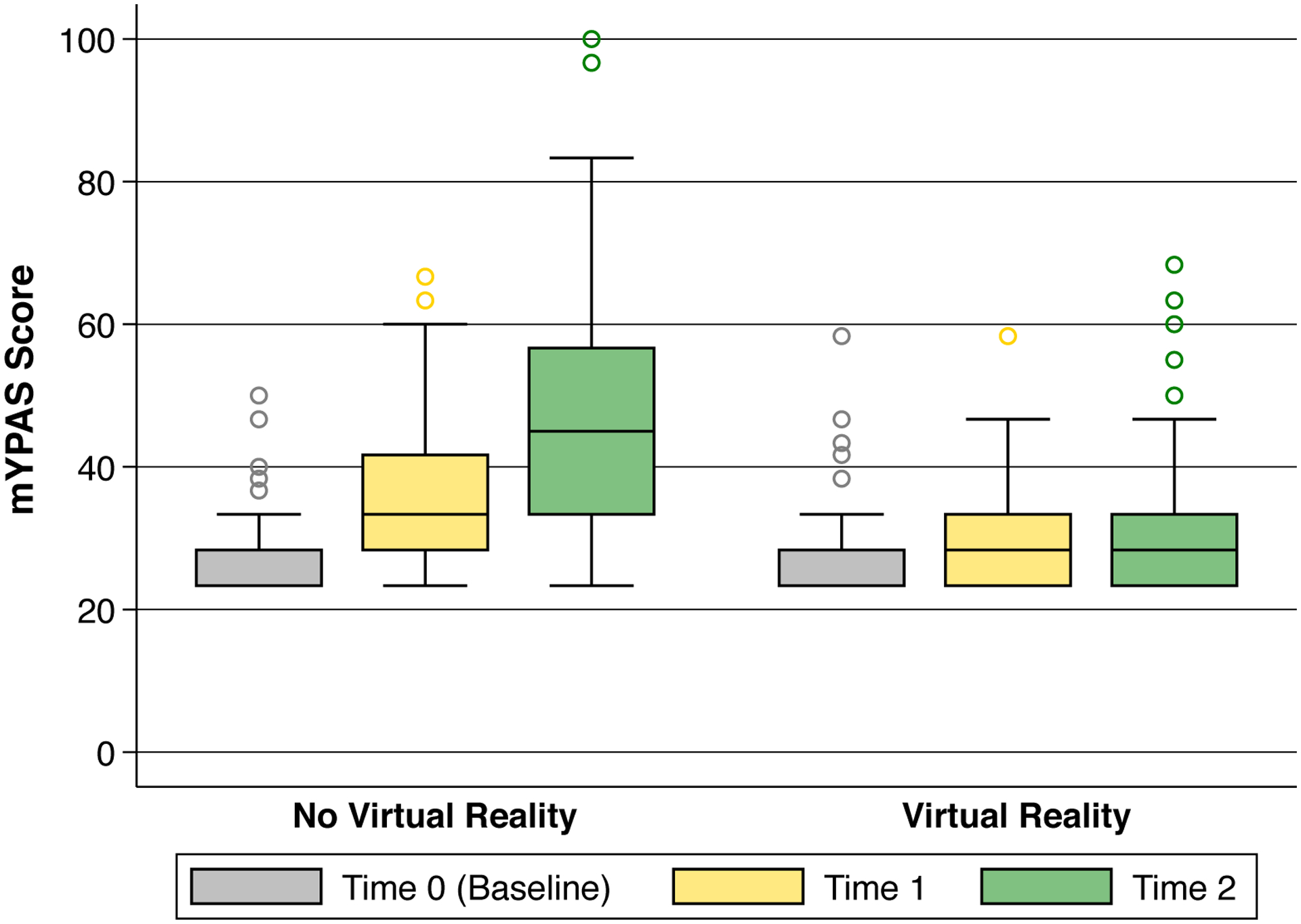
Methods: In this randomized-controlled, parallel-group study, 71 children 5-12 years of age scheduled for elective surgery with GA were randomly allocated to a VR group or a non-VR (No VR) control group. VR group patients underwent audiovisual distraction with a VR headset during induction in the operating room, whereas the control group received no audiovisual distraction. The primary outcome was the Modified Yale Preoperative Anxiety Scale (mYPAS), which was measured at 3 time points to assess patient anxiety: in the preoperative holding area before randomization, on entering the operating room, and during induction of GA. The primary outcome was analyzed using univariate analysis and a linear mixed-effects model. Secondary outcomes included postinduction parental anxiety measured by the State-Trait Anxiety Inventory, pediatric induction compliance, and parental satisfaction.
Results: Average patient age was 8.0 ± 2.3 years (mean ± standard deviation [SD]), and 51.4% of patients were female. Baseline variables were not substantially different between the VR group (33 patients) and the No VR group (37 patients). No patients received preoperative anxiolytic medication. Baseline mYPAS scores were not different between the groups, with scores of 28.3 (23.3-28.3) (median [interquartile range {IQR}]) in both. The change in mYPAS scores from baseline to time of induction was significantly lower in the VR group versus control group (0.0 [0.0-5.0] vs 13.3 [5.0-26.7]; P < .0001). In the mixed-effects model, the VR group had an estimated 6.0-point lower mYPAS score (95% confidence interval [CI], 0.7-11.3; P = .03) at room entry than the No VR group, and 14.5-point lower score (95% CI, 9.3-19.8; P < .0001) at induction versus control. Randomization to VR did not alter parental anxiety (0 [-2 to 2]), pediatric induction compliance (0 [0-0]), or parental satisfaction (-3 [-8 to 2]) (difference in medians [95% CI]).
Conclusions: This study demonstrates a reduction in pediatric preoperative anxiety with the use of VR. Preoperative VR may be an effective noninvasive modality for anxiolysis during induction of anesthesia in children.
Trial registration: ClinicalTrials.gov NCT03583450.
Copyright © 2020 International Anesthesia Research Society.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures

References
-
- Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative anxiety in children. Predictors and outcomes. Arch Pediatr Adolesc Med. 1996;150:1238–1245. - PubMed
-
- Davidson AJ, Shrivastava PP, Jamsen K, et al. Risk factors for anxiety at induction of anesthesia in children: a prospective cohort study. Paediatr Anaesth. 2006;16:919–927. - PubMed
-
- Kain ZN, Wang SM, Mayes LC, Caramico LA, Hofstadter MB. Distress during the induction of anesthesia and postoperative behavioral outcomes. Anesth Analg. 1999;88:1042–1047. - PubMed
-
- Kain ZN, Mayes LC, Caldwell-Andrews AA, Karas DE, McClain BC. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics. 2006;118:651–658. - PubMed
