

Evaluating the Clinical Impact of Rapid Response Electroencephalography: The DECIDE Multicenter Prospective Observational Clinical Study
- PMID: 32618687
- PMCID: PMC7735649
- DOI: 10.1097/CCM.0000000000004428
Evaluating the Clinical Impact of Rapid Response Electroencephalography: The DECIDE Multicenter Prospective Observational Clinical Study
Abstract
Objectives: To measure the diagnostic accuracy, timeliness, and ease of use of Ceribell rapid response electroencephalography. We assessed physicians' diagnostic assessments and treatment plans before and after rapid response electroencephalography assessment. Primary outcomes were changes in physicians' diagnostic and therapeutic decision making and their confidence in these decisions based on the use of the rapid response electroencephalography system. Secondary outcomes were time to electroencephalography, setup time, ease of use, and quality of electroencephalography data.
Design: Prospective multicenter nonrandomized observational study.
Setting: ICUs in five academic hospitals in the United States.
Subjects: Patients with encephalopathy suspected of having nonconvulsive seizures and physicians evaluating these patients.
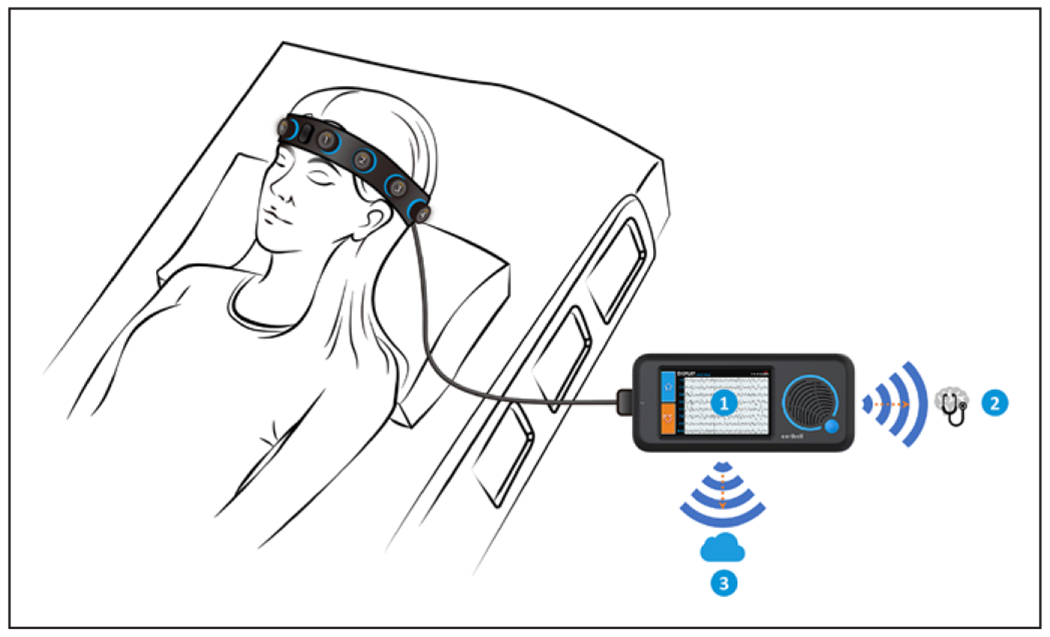
Interventions: Physician bedside assessment of sonified electroencephalography (30 s from each hemisphere) and visual electroencephalography (60 s) using rapid response electroencephalography.
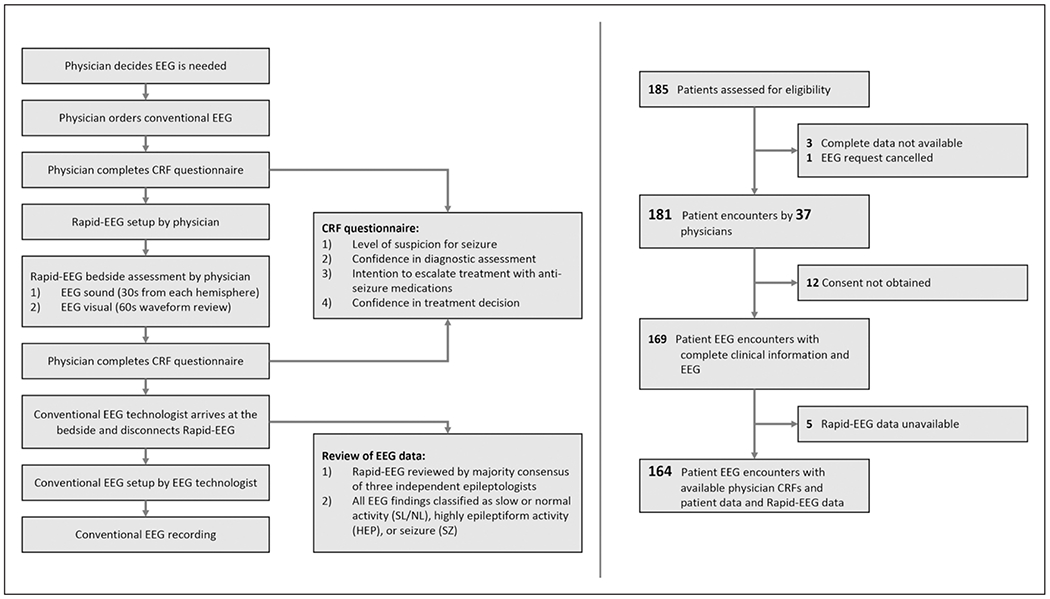
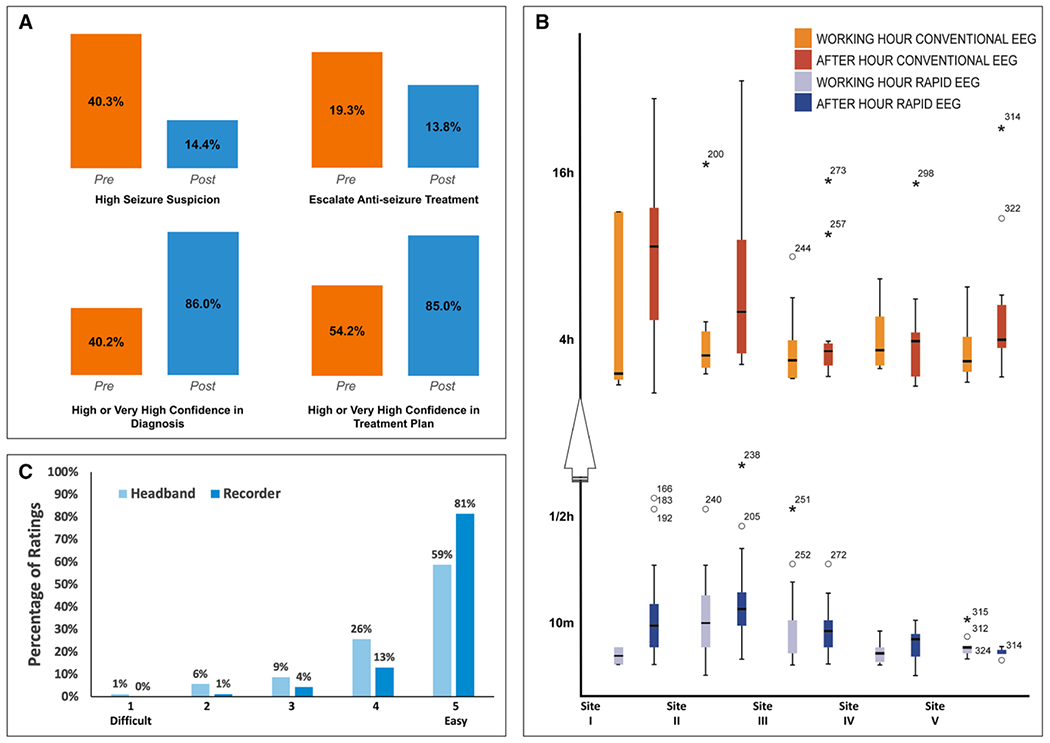
Measurements and main results: Physicians (29 fellows or residents, eight attending neurologists) evaluated 181 ICU patients; complete clinical and electroencephalography data were available in 164 patients (average 58.6 ± 18.7 yr old, 45% females). Relying on rapid response electroencephalography information at the bedside improved the sensitivity (95% CI) of physicians' seizure diagnosis from 77.8% (40.0%, 97.2%) to 100% (66.4%, 100%) and the specificity (95% CI) of their diagnosis from 63.9% (55.8%, 71.4%) to 89% (83.0%, 93.5%). Physicians' confidence in their own diagnosis and treatment plan were also improved. Time to electroencephalography (median [interquartile range]) was 5 minutes (4-10 min) with rapid response electroencephalography while the conventional electroencephalography was delayed by several hours (median [interquartile range] delay = 239 minutes [134-471 min] [p < 0.0001 using Wilcoxon signed rank test]). The device was rated as easy to use (mean ± SD: 4.7 ± 0.6 [1 = difficult, 5 = easy]) and was without serious adverse effects.
Conclusions: Rapid response electroencephalography enabled timely and more accurate assessment of patients in the critical care setting. The use of rapid response electroencephalography may be clinically beneficial in the assessment of patients with high suspicion for nonconvulsive seizures and status epilepticus.
Trial registration: ClinicalTrials.gov NCT03534258.
Figures
Comment in
-
Sonification of Seizures: Music to Our Ears.Crit Care Med. 2020 Sep;48(9):1383-1385. doi: 10.1097/CCM.0000000000004483. Crit Care Med. 2020. PMID: 32826490 No abstract available.
References
-
- DeLorenzo RJ, Waterhouse EJ, Towne AR, et al.: Persistent nonconvulsive status epilepticus after the control of convulsive status epilepticus. Epilepsia 1998; 39:833–840 - PubMed
-
- Ronne-Engstrom E, Winkler T: Continuous EEG monitoring in patients with traumatic brain injury reveals a high incidence of epileptiform activity. Acta Neurol Scand 2006; 114:47–53 - PubMed
-
- Little AS, Kerrigan JF, McDougall CG, et al.: Nonconvulsive status epilepticus in patients suffering spontaneous subarachnoid hemorrhage. J Neurosurg 2007; 106:805–811 - PubMed
-
- Claassen J, Peery S, Kreiter KT, et al.: Predictors and clinical impact of epilepsy after subarachnoid hemorrhage. Neurology 2003; 60:208–214 - PubMed
