

The Impact of Vaccination Efforts on the Spatiotemporal Patterns of the Hepatitis A Outbreak in Michigan, 2016-2018
- PMID: 32618711
- PMCID: PMC7444463
- DOI: 10.1097/EDE.0000000000001218
The Impact of Vaccination Efforts on the Spatiotemporal Patterns of the Hepatitis A Outbreak in Michigan, 2016-2018
Abstract
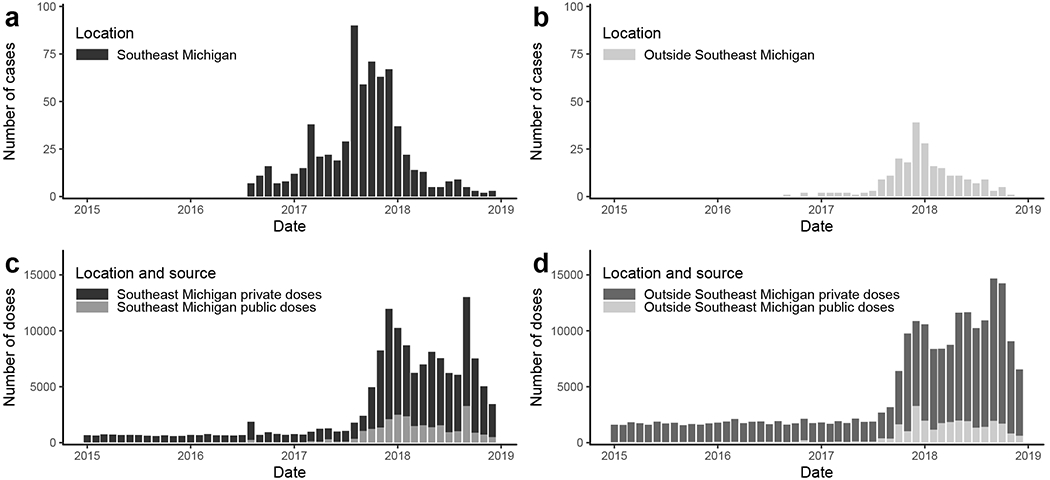
Background: The United States is currently experiencing the largest hepatitis A virus (HAV) outbreak since the introduction of a vaccine in 1996. More than 31,000 cases have been reported since 2016. Although HAV had largely been considered a foodborne pathogen in recent years, this outbreak has been spread primarily through person-to-person transmission in urban settings and has been associated with homelessness and substance use. Michigan was one of the first states to report an outbreak, with 910 reported cases between August 2016 and December 2018.
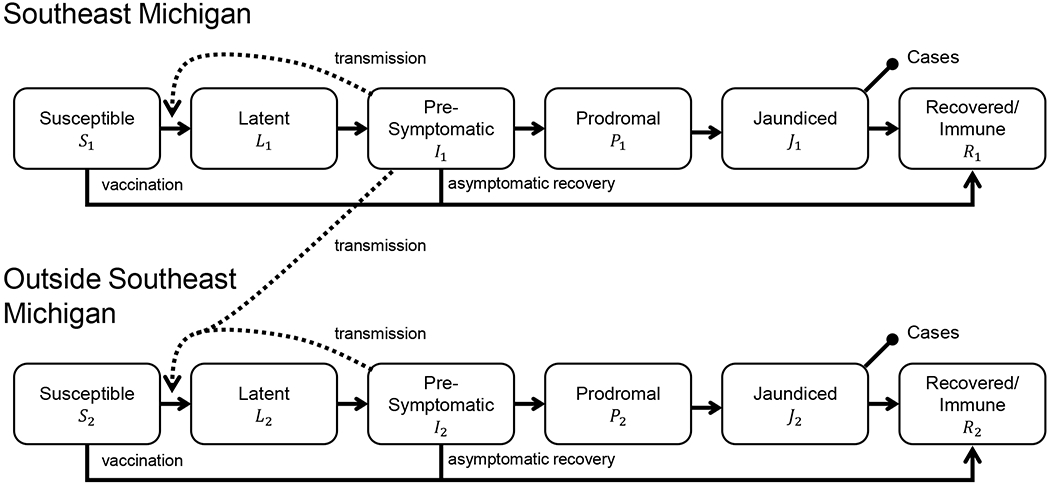
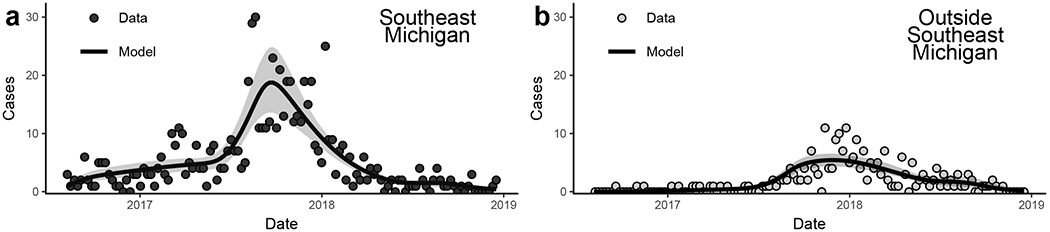
Methods: We analyzed surveillance and vaccination data from Michigan using a disease transmission model to investigate how vaccine timing and coverage influenced the spatiotemporal patterns of the outbreak, distinguishing between Southeast Michigan, where the outbreak began, and the rest of the state.
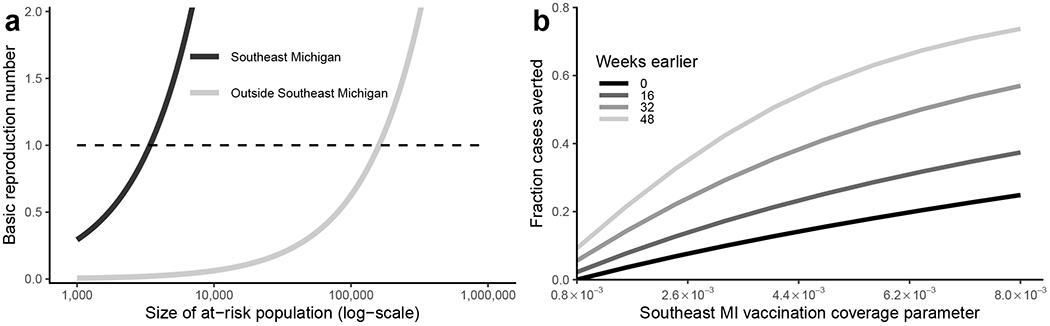
Results: We estimated that vaccination had little impact in Southeast Michigan (3% cases averted [95% confidence interval (CI) = 1%, 8%]) but had a substantial impact in the rest of the state, preventing a larger outbreak (91% cases averted [95% CI = 85%, 97%]) lasting several more years.
Conclusions: Our results emphasize the value of targeting populations where local transmission is not yet sustained rather than populations where transmission is already waning. Simulation modeling can aid in proactive rather than reactive decision-making and may help direct the response to outbreaks emerging in other states. See video abstract: http://links.lww.com/EDE/B704.
Figures
References
-
- Wasley A, Samandari T, Bell BP. Incidence of hepatitis A in the United States in the era of vaccination. Journal of the American Medical Association. 2005;294(2):194–201. - PubMed
-
- Murphy TV, Denniston MM, Hill HA, McDonald M, Klevens MR, Elam-Evans LD, et al. Progress Toward Eliminating Hepatitis A Disease in the United States. Morbidity and Mortality Weekly Report Supplements. 2016;65(1):29–41. - PubMed
-
- Ashur Y, Adler R, Rowe M, Shouval D. Comparison of immunogenicity of two hepatitis A vaccines - VAQTA® and HAVRIX® - in young adults. Vaccine. 1999;17(18):2290–2296. - PubMed
-
- Demicheli V, Tiberti D. The effectiveness and safety of hepatitis A vaccine: A systematic review. Vaccine. 2003;21(19-20):2242–2245. - PubMed
-
- Sharapov UM, Bulkow LR, Negus SE, Spradling PR, Homan C, Drobeniuc J, et al. Persistence of hepatitis A vaccine induced seropositivity in infants and young children by maternal antibody status: 10-year follow-up. Hepatology. 2012;56(2):516–522. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
