

SARS-CoV-2 Impact on Elective Orthopaedic Surgery: Implications for Post-Pandemic Recovery
- PMID: 32618916
- PMCID: PMC7396217
- DOI: 10.2106/JBJS.20.00602
SARS-CoV-2 Impact on Elective Orthopaedic Surgery: Implications for Post-Pandemic Recovery
Abstract
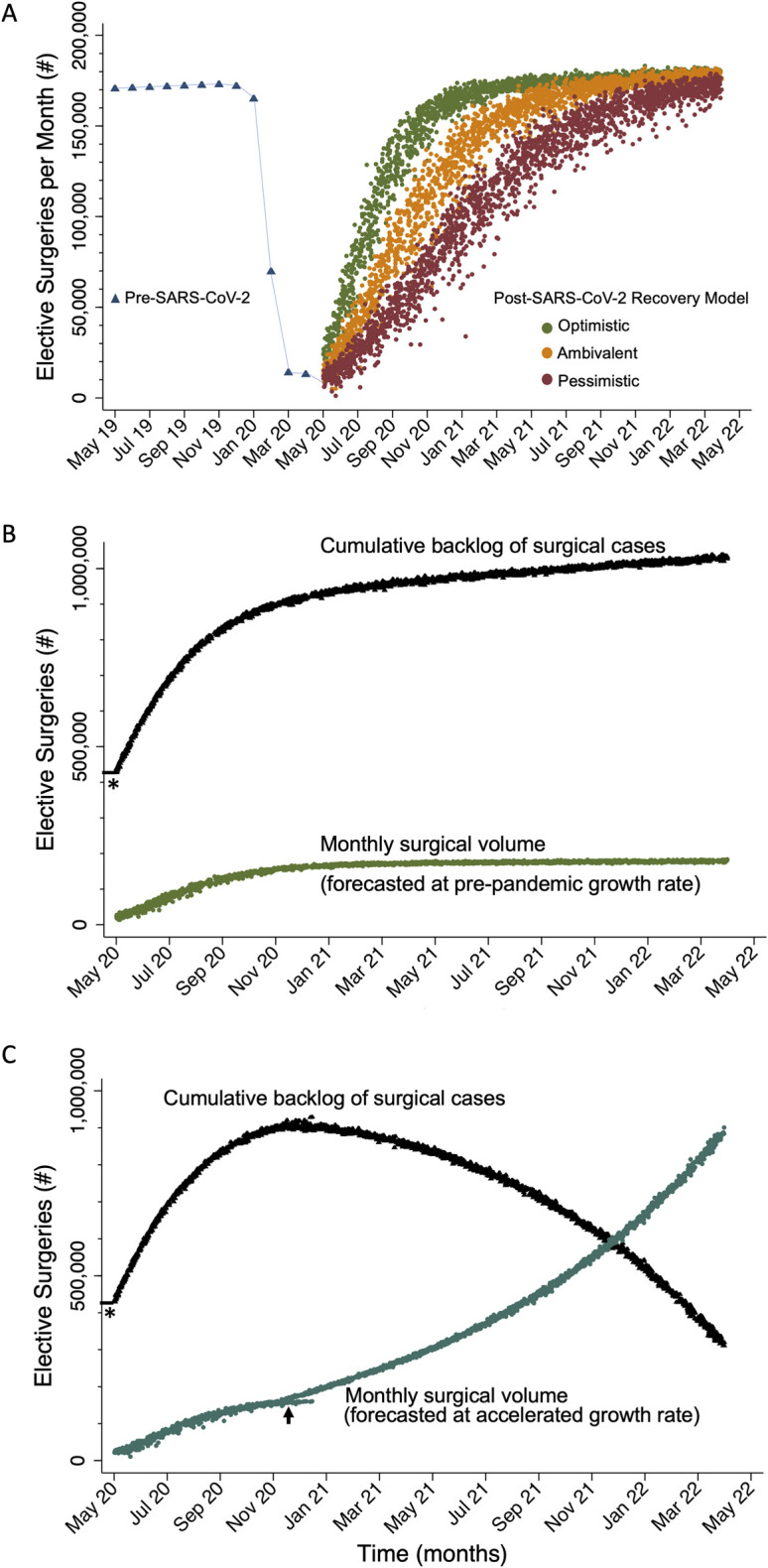
Background: The aim of our study was to explore the impact of elective-surgery deferment on the United States health-care system and subsequent recovery after COVID-19 containment. Using an orthopaedic elective surgery model, we aimed to answer the following: (1) What is the expected recovery time until the health-care system is back to nearly full capacity for performing elective surgery? (2) What will be the expected backlog of elective surgery over time? (3) How should health care change to address the backlog?
Methods: A Monte Carlo stochastic simulation-based analysis was performed to forecast the post-pandemic volume of elective, inpatient total joint arthroplasty and spinal fusion surgical cases. The cumulative backlog was calculated and analyzed. We tested model assumptions with sensitivity analyses.
Results: Assuming that elective orthopaedic surgery resumes in June 2020, it will take 7, 12, and 16 months-in optimistic, ambivalent, and pessimistic scenarios, respectively-until the health-care system can perform 90% of the expected pre-pandemic forecasted volume of surgery. In the optimistic scenario, there will be a cumulative backlog of >1 million surgical cases at 2 years after the end of elective-surgery deferment.
Conclusions: The deferment of elective surgical cases during the SARS-CoV-2 pandemic will have a lasting impact on the United States health-care system. As part of disaster mitigation, it is critical to start planning for recovery now.
Figures
References
-
- Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. National Inpatient Sample (NIS) data 1993-2017.
-
- Cobb CW, Douglas PH. A theory of production. Am Econ Rev. 1928. March;18(1):139-1-5.
-
- Sloan M, Premkumar A, Sheth NP. Projected volume of primary total joint arthroplasty in the U.S., 2014 to 2030. J Bone Joint Surg Am. 2018. September 5;100(17):1455-1-5. - PubMed
-
- Riganti A, Siciliani L, Fiorio CV. The effect of waiting times on demand and supply for elective surgery: evidence from Italy. Health Econ. 2017. September;26(Suppl 2):92-1-5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
