

Regional adiposity and heart failure with preserved ejection fraction
- PMID: 32619081
- PMCID: PMC9991865
- DOI: 10.1002/ejhf.1956
Regional adiposity and heart failure with preserved ejection fraction
Abstract
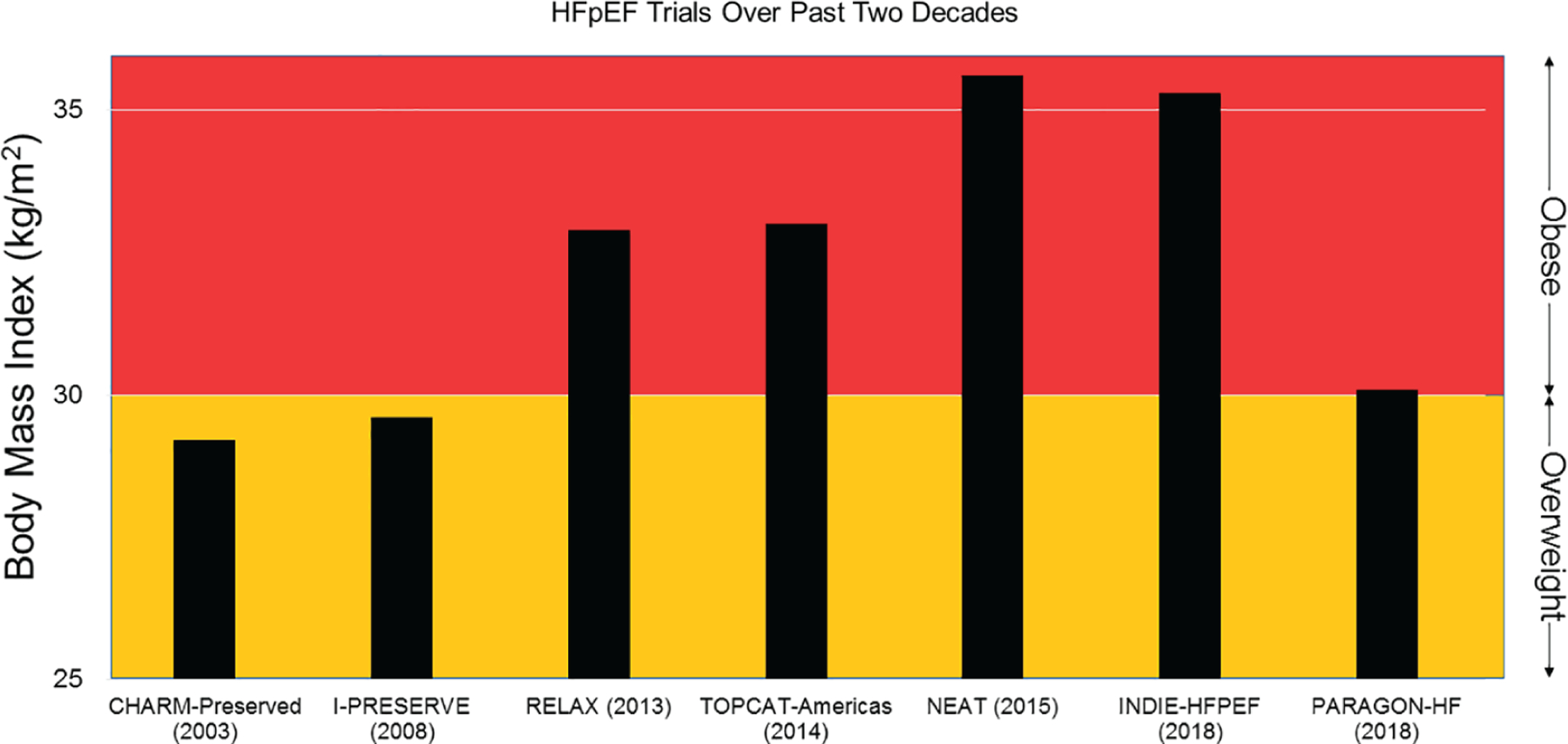
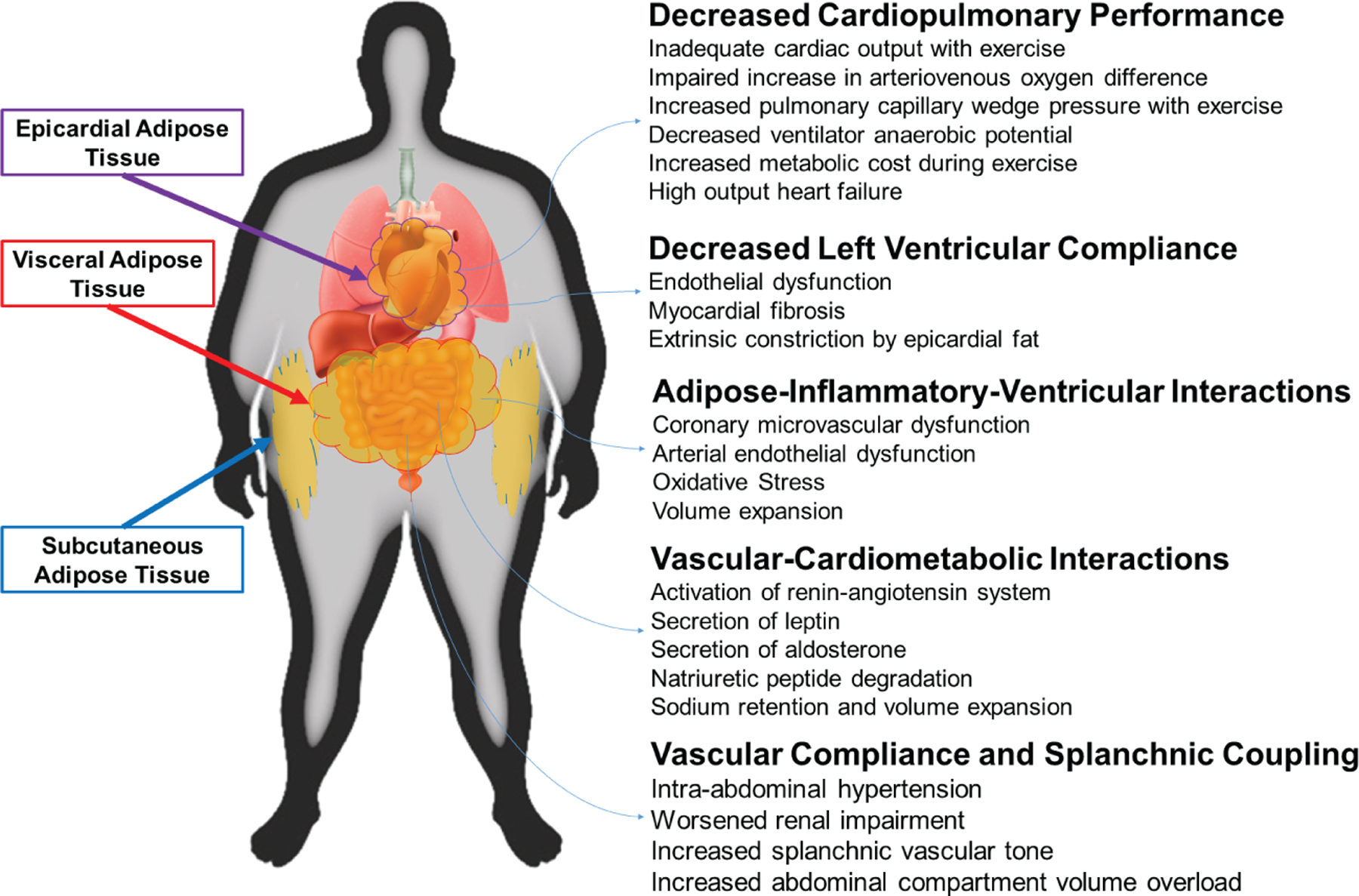
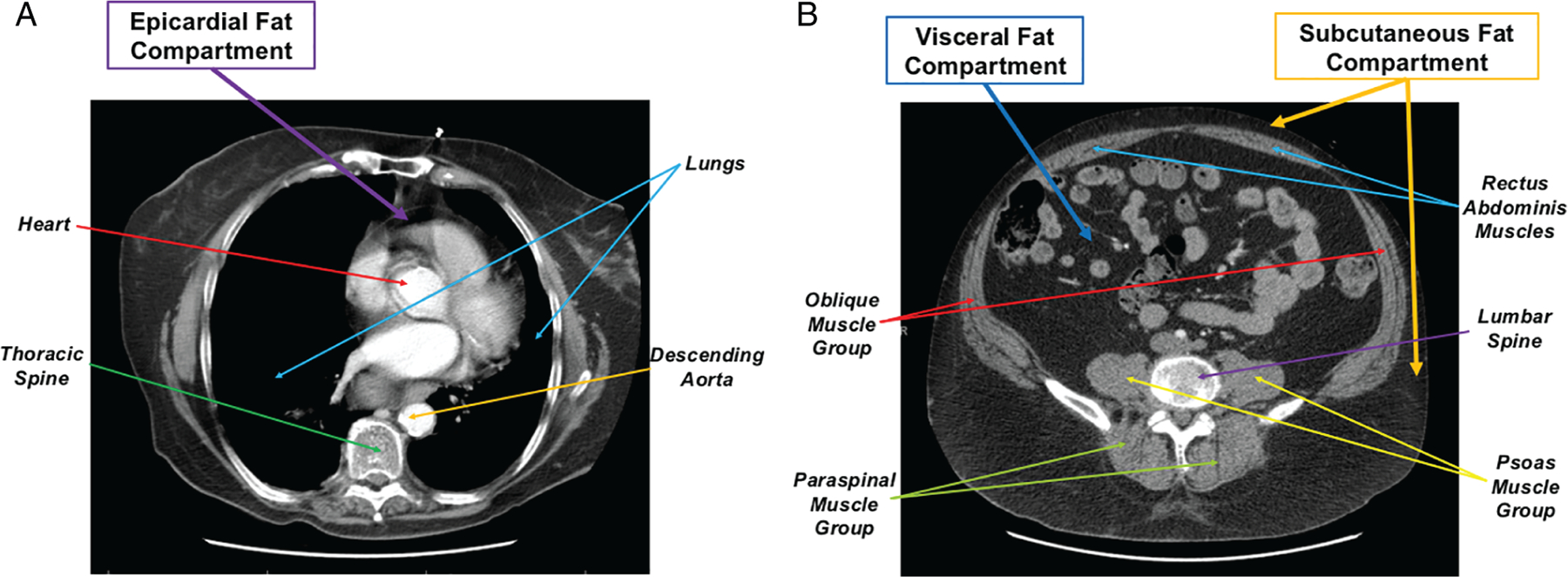
The role of obesity in the pathogenesis of heart failure (HF), and in particular HF with preserved ejection fraction (HFpEF), has drawn significant attention in recent years. The prevalence of both obesity and HFpEF has increased worldwide over the past decades and when present concomitantly suggests an obese-HFpEF phenotype. Anthropometrics, including body mass index, waist circumference, and waist-to-hip ratio, are associated with incident HFpEF. However, the cardiovascular effects of obesity may actually be driven by the distribution of fat, which can accumulate in the epicardial, visceral, and subcutaneous compartments. Regional fat can be quantified using non-invasive imaging techniques, including computed tomography, magnetic resonance imaging, and dual-energy X-ray absorptiometry. Regional variations in fat accumulation are associated with different HFpEF risk profiles, whereby higher epicardial and visceral fat have a much stronger association with HFpEF risk compared with elevated subcutaneous fat. Thus, regional adiposity may serve a pivotal role in the pathophysiology of HFpEF contributing to decreased cardiopulmonary fitness, impaired left ventricular compliance, upregulation of local and systemic inflammation, promotion of neurohormonal dysregulation, and increased intra-abdominal pressure and vascular congestion. Strategies to reduce total and regional adiposity have shown promise, including intensive exercise, dieting, and bariatric surgery programmes, but few studies have focused on HFpEF-related outcomes among obese. Further understanding the role these variable fat depots play in the progression of HFpEF and HFpEF-related hospitalizations may provide therapeutic targets in treating the obese-HFpEF phenotype.
Keywords: Heart failure; Heart failure with preserved ejection fraction; Obesity; Regional adiposity.
© 2020 European Society of Cardiology.
Conflict of interest statement
Figures
References
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Køber L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rønnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A; ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14: 803–869. - PubMed
-
- Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, Hernandez AF, Fonarow GC; Get With the Guidelines Scientific Advisory Committee and Investigators. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation 2012;126:65–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
