

A risk calculator to inform the need for a prostate biopsy: a rapid access clinic cohort
- PMID: 32620120
- PMCID: PMC7333322
- DOI: 10.1186/s12911-020-01174-2
A risk calculator to inform the need for a prostate biopsy: a rapid access clinic cohort
Abstract
Background: Prostate cancer (PCa) represents a significant healthcare problem. The critical clinical question is the need for a biopsy. Accurate risk stratification of patients before a biopsy can allow for individualised risk stratification thus improving clinical decision making. This study aims to build a risk calculator to inform the need for a prostate biopsy.
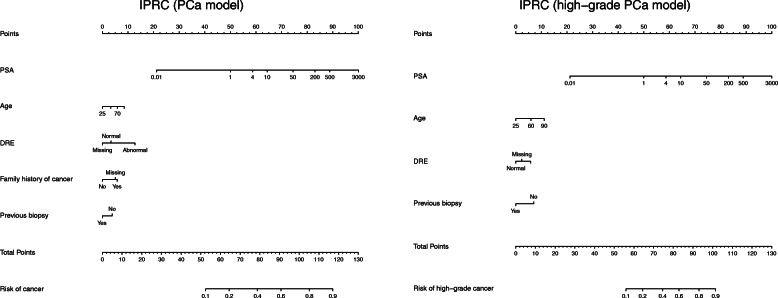
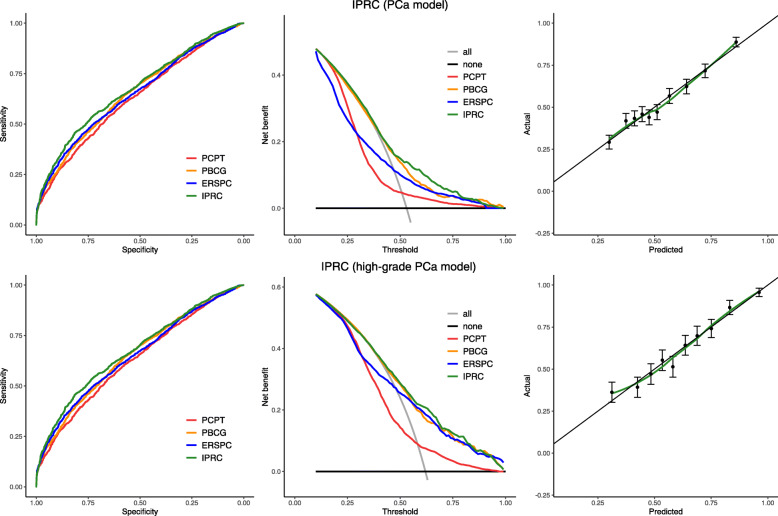
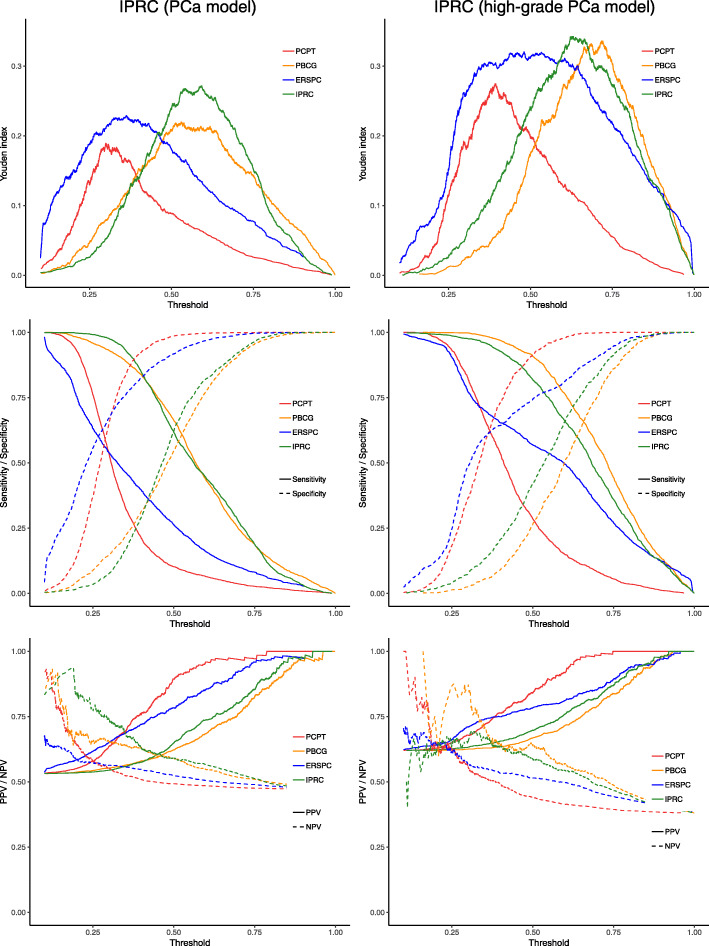
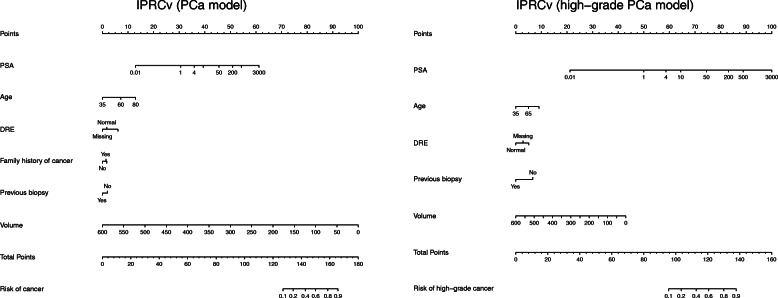
Methods: Using the clinical information of 4801 patients an Irish Prostate Cancer Risk Calculator (IPRC) for diagnosis of PCa and high grade (Gleason ≥7) was created using a binary regression model including age, digital rectal examination, family history of PCa, negative prior biopsy and Prostate-specific antigen (PSA) level as risk factors. The discrimination ability of the risk calculator is internally validated using cross validation to reduce overfitting, and its performance compared with PSA and the American risk calculator (PCPT), Prostate Biopsy Collaborative Group (PBCG) and European risk calculator (ERSPC) using various performance outcome summaries. In a subgroup of 2970 patients, prostate volume was included. Separate risk calculators including the prostate volume (IPRCv) for the diagnosis of PCa (and high-grade PCa) was created.
Results: IPRC area under the curve (AUC) for the prediction of PCa and high-grade PCa was 0.6741 (95% CI, 0.6591 to 0.6890) and 0.7214 (95% CI, 0.7018 to 0.7409) respectively. This significantly outperforms the predictive ability of cancer detection for PSA (0.5948), PCPT (0.6304), PBCG (0.6528) and ERSPC (0.6502) risk calculators; and also, for detecting high-grade cancer for PSA (0.6623) and PCPT (0.6804) but there was no significant improvement for PBCG (0.7185) and ERSPC (0.7140). The inclusion of prostate volume into the risk calculator significantly improved the AUC for cancer detection (AUC = 0.7298; 95% CI, 0.7119 to 0.7478), but not for high-grade cancer (AUC = 0.7256; 95% CI, 0.7017 to 0.7495). The risk calculator also demonstrated an increased net benefit on decision curve analysis.
Conclusion: The risk calculator developed has advantages over prior risk stratification of prostate cancer patients before the biopsy. It will reduce the number of men requiring a biopsy and their exposure to its side effects. The interactive tools developed are beneficial to translate the risk calculator into practice and allows for clarity in the clinical recommendations.
Keywords: Binary logistic regression, cross-validation, Rshiny; Biopsy; Decision-making; Prostate Cancer; Risk calculator.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- National Cancer Registry (2014) Cancer in Ireland 1994–2011: Annual report of the National Cancer Registry 2014. http://www.ncri.ie/sites/ncri/files/pubs/annual report 2014.pdf. Accessed 2 Jul 2014.
-
- National Cancer Registry (2010) Cancer Trends. No. 3. Recent trends in prostate cancer.
-
- Lee KL, Woodlief LH, Topol EJ, Weaver WD, Betriu A, Col J, et al. Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I investigators. Circulation. 1995;91:1659–1668. doi: 10.1161/01.CIR.91.6.1659. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
