

A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale
- PMID: 32621759
- PMCID: PMC7689909
- DOI: 10.1002/ijc.33185
A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale
Abstract
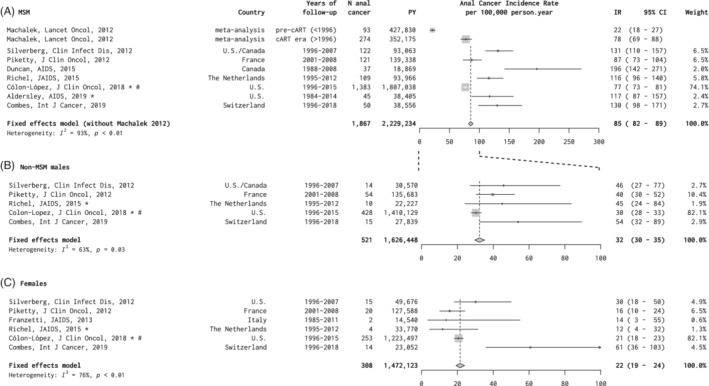
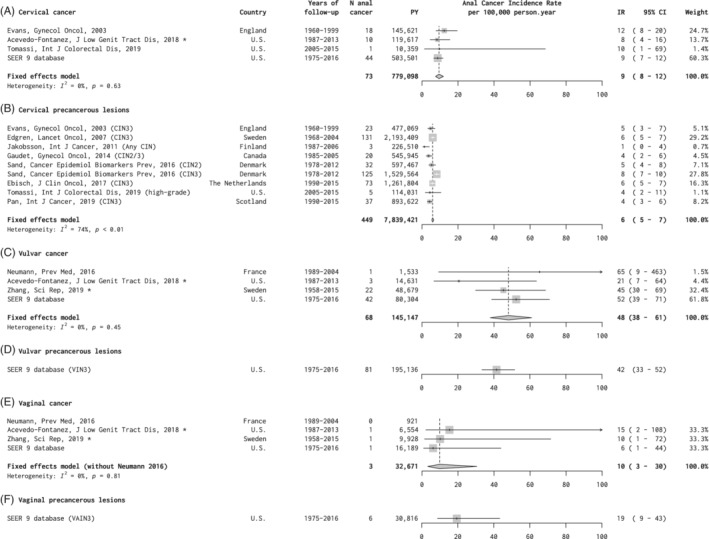
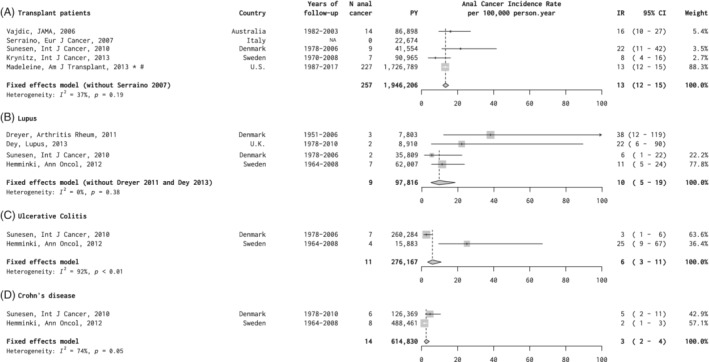
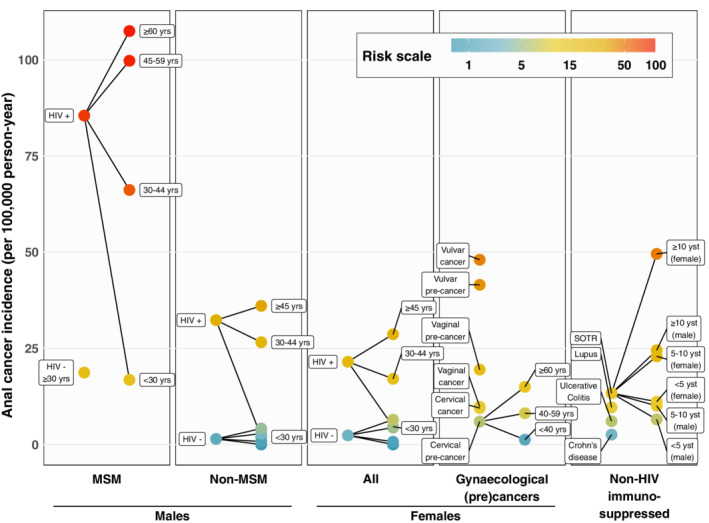
Certain population groups are known to have higher than average anal cancer risk, namely persons living with HIV (PLHIV), men who have sex with men (MSM), women diagnosed with human papillomavirus (HPV)-related gynecological precancerous lesions or cancer, solid organ transplant recipients (SOTRs) and patients with autoimmune diseases. Our aim was to provide robust and comparable estimates of anal cancer burden across these groups. Summary incidence rates (IRs), as cases per 100 000 person-years (py), were calculated by fixed-effects meta-analysis. IRs were 85 (95% confidence interval [CI] = 82-89) for HIV-positive MSM (n = 7 studies; 2 229 234 py), 32 (95% CI = 30-35) for non-MSM male PLHIV (n = 5; 1626 448 py) and 22 (95% CI = 19-24) for female PLHIV (n = 6; 1 472 123 py), with strong variation by age (eg, from 16.8 < 30 years to 107.5 ≥ 60 years for HIV-positive MSM). IR was 19 (95% CI = 10-36) in HIV-negative MSM (n = 2; 48 135 py). Anal cancer IRs were much higher after diagnosis of vulvar (IR = 48 [95% CI = 38-61]; n = 4; 145 147 py) than cervical (9 [95% CI = 8-12]; n = 4; 779 098 py) or vaginal (IR = 10 [95% CI = 3-30]; n = 4; 32 671) cancer, with equivalent disparity after respective precancerous lesions. IR was 13 (95% CI = 12-15) in SOTRs (n = 5; 1 946 206 py), reaching 24.5 and 49.6 for males and females >10 years after transplant. Anal cancer IRs were 10 (95% CI = 5-19), 6 (95% CI = 3-11) and 3 (95% CI = 2-4) for systemic lupus erythematosus, ulcerative colitis and Crohn's disease, respectively. In conclusion, a unifying anal cancer risk scale, based upon comprehensive meta-analysis, can improve prioritization and standardization in anal cancer prevention/research initiatives, which are in their public health infancy.
Keywords: HIV; MSM; anal cancer; incidence; transplantation.
© 2020 International Agency for Research on Cancer (IARC/WHO); licensed by John Wiley & Sons Ltd on behalf of Union for International Cancer Control.
Conflict of interest statement
E.A.S. reports personal fees from Physicians Research Network, personal fees and nonfinancial support from British Association for Sexual Health and HIV, nonfinancial support from Eurogin, personal fees and nonfinancial support from ASCCP, outside the submitted work. The other authors declare no conflicts of interest.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
