

COVID-19 in health-care workers in three hospitals in the south of the Netherlands: a cross-sectional study
- PMID: 32622380
- PMCID: PMC7332281
- DOI: 10.1016/S1473-3099(20)30527-2
COVID-19 in health-care workers in three hospitals in the south of the Netherlands: a cross-sectional study
Erratum in
-
Correction to Lancet Infect Dis 2020; published online July 2. https://doi.org/10.1016/S1473-3099(20)30527-2.Lancet Infect Dis. 2020 Sep;20(9):e215. doi: 10.1016/S1473-3099(20)30608-3. Epub 2020 Aug 3. Lancet Infect Dis. 2020. PMID: 32758437 Free PMC article. No abstract available.
Abstract
Background: 10 days after the first reported case of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in the Netherlands (on Feb 27, 2020), 55 (4%) of 1497 health-care workers in nine hospitals located in the south of the Netherlands had tested positive for SARS-CoV-2 RNA. We aimed to gain insight in possible sources of infection in health-care workers.
Methods: We did a cross-sectional study at three of the nine hospitals located in the south of the Netherlands. We screened health-care workers at the participating hospitals for SARS-CoV-2 infection, based on clinical symptoms (fever or mild respiratory symptoms) in the 10 days before screening. We obtained epidemiological data through structured interviews with health-care workers and combined this information with data from whole-genome sequencing of SARS-CoV-2 in clinical samples taken from health-care workers and patients. We did an in-depth analysis of sources and modes of transmission of SARS-CoV-2 in health-care workers and patients.
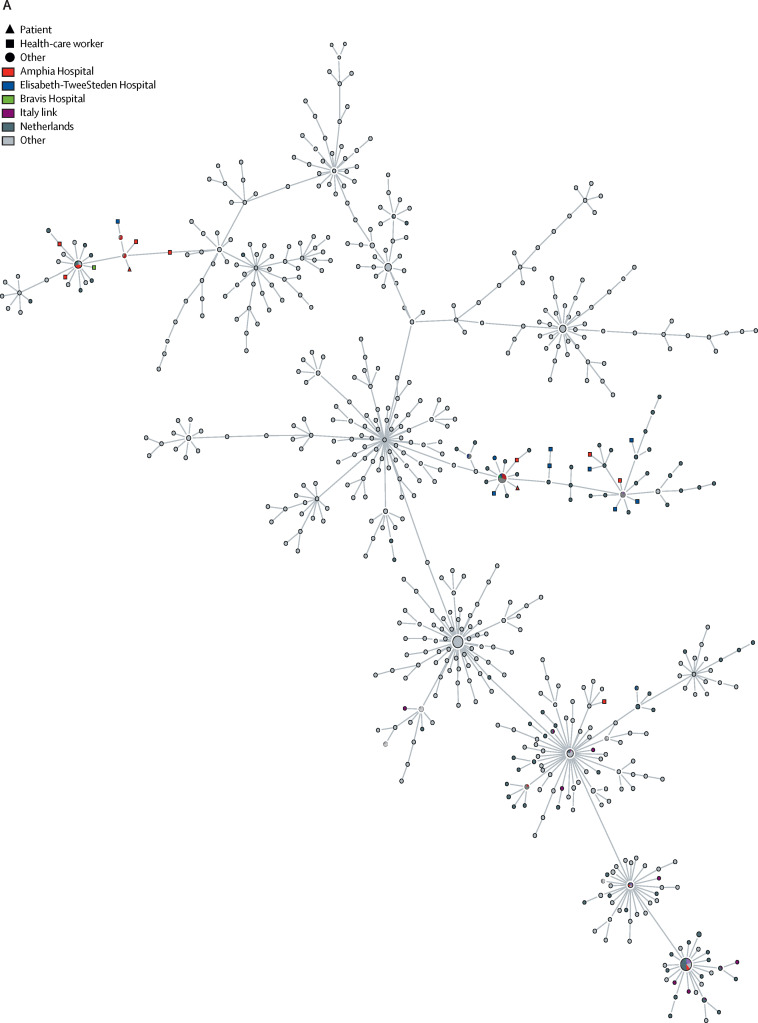
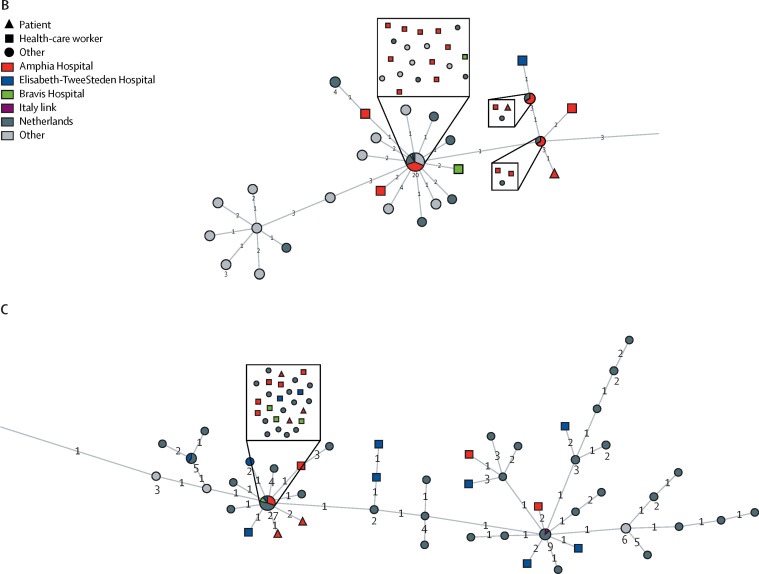
Findings: Between March 2 and March 12, 2020, 1796 (15%) of 12 022 health-care workers were screened, of whom 96 (5%) tested positive for SARS-CoV-2. We obtained complete and near-complete genome sequences from 50 health-care workers and ten patients. Most sequences were grouped in three clusters, with two clusters showing local circulation within the region. The noted patterns were consistent with multiple introductions into the hospitals through community-acquired infections and local amplification in the community.
Interpretation: Although direct transmission in the hospitals cannot be ruled out, our data do not support widespread nosocomial transmission as the source of infection in patients or health-care workers.
Funding: EU Horizon 2020 (RECoVer, VEO, and the European Joint Programme One Health METASTAVA), and the National Institute of Allergy and Infectious Diseases, National Institutes of Health.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- WHO Report of the WHO–China Joint Mission on Coronavirus Disease 2019 (COVID-19) Feb 28, 2020. https://www.who.int/publications/i/item/report-of-the-who-china-joint-mi...
-
- WHO Regional Office for the Eastern Mediterranean MERS situation update. January, 2020. http://www.emro.who.int/pandemic-epidemic-diseases/mers-cov/mers-situati...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
