

Early CD4+ T cell reconstitution as predictor of outcomes after allogeneic hematopoietic cell transplantation
- PMID: 32622752
- PMCID: PMC7484404
- DOI: 10.1016/j.jcyt.2020.05.005
Early CD4+ T cell reconstitution as predictor of outcomes after allogeneic hematopoietic cell transplantation
Abstract
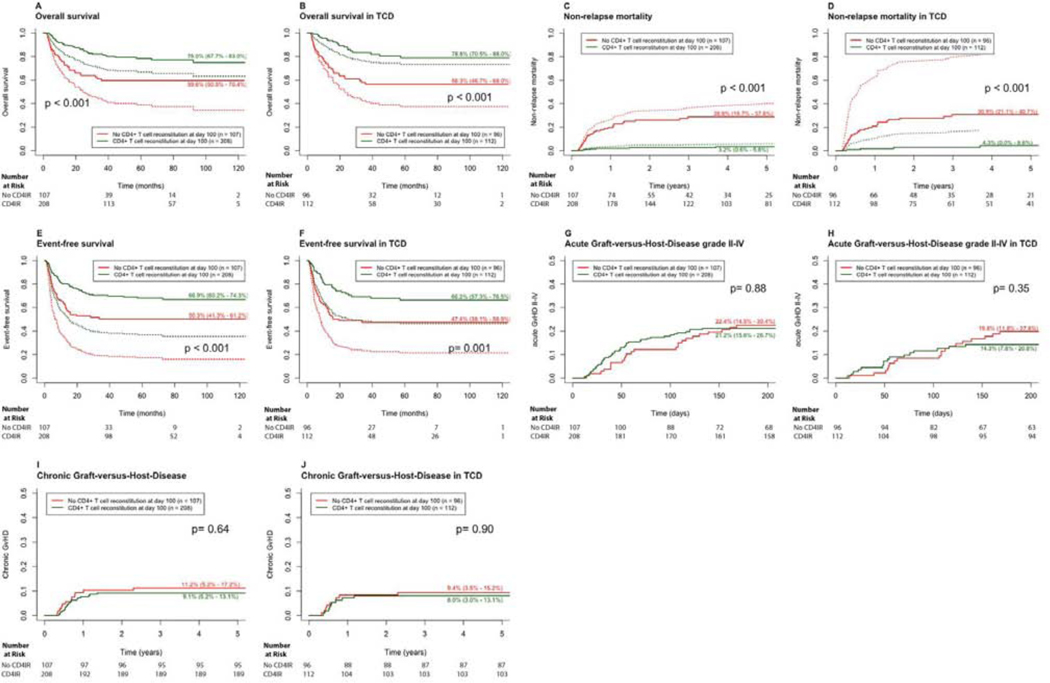
Background: An association between early CD4+ T cell immune reconstitution (CD4+ IR) and survival after T-replete allogeneic hematopoietic cell transplantation (HCT) has been previously reported. Here we report validation of this relationship in a separate cohort that included recipients of ex vivo T-cell-depleted (TCD) HCT. We studied the relationship between CD4+ IR and clinical outcomes.
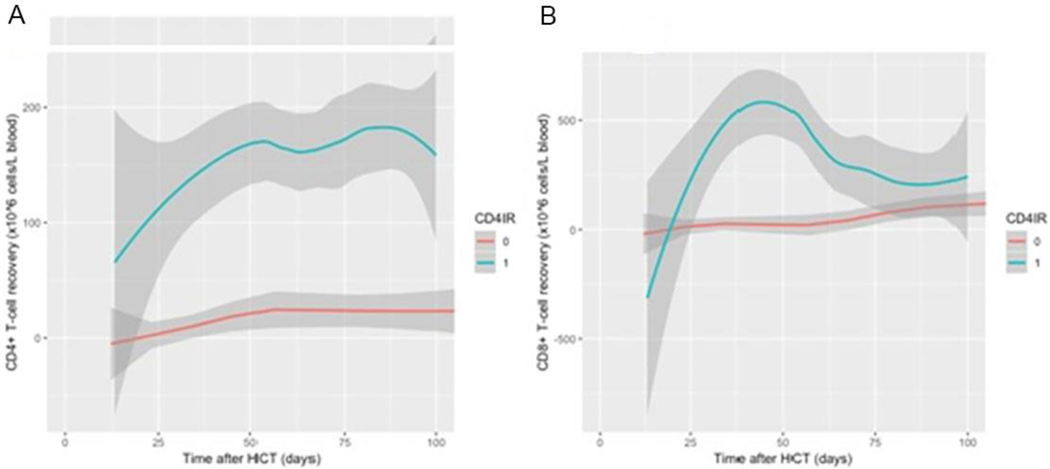
Methods: A retrospective analysis of children/young adults receiving their first allogeneic HCT for any indication between January 2008 and December 2017 was performed. We related early CD4+ IR (defined as achieving >50 CD4+ T cells/µL on two consecutive measures within 100 days of HCT) to overall survival (OS), relapse, non-relapse mortality (NRM), event-free survival (EFS) and acute graft-versus-host disease (aGVHD). Fine and Gray competing risk models and Cox proportional hazard models were used.
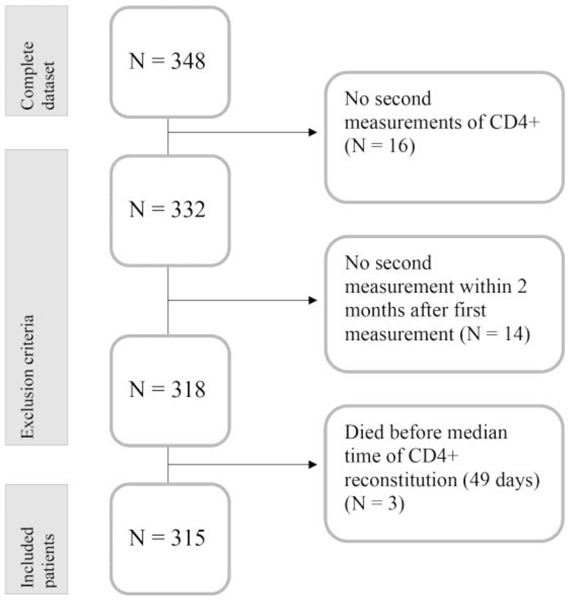
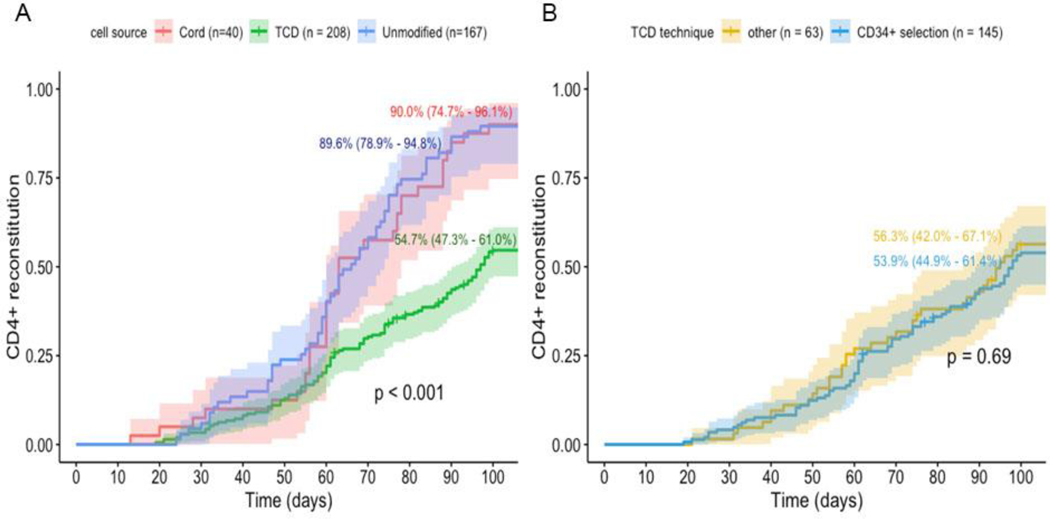
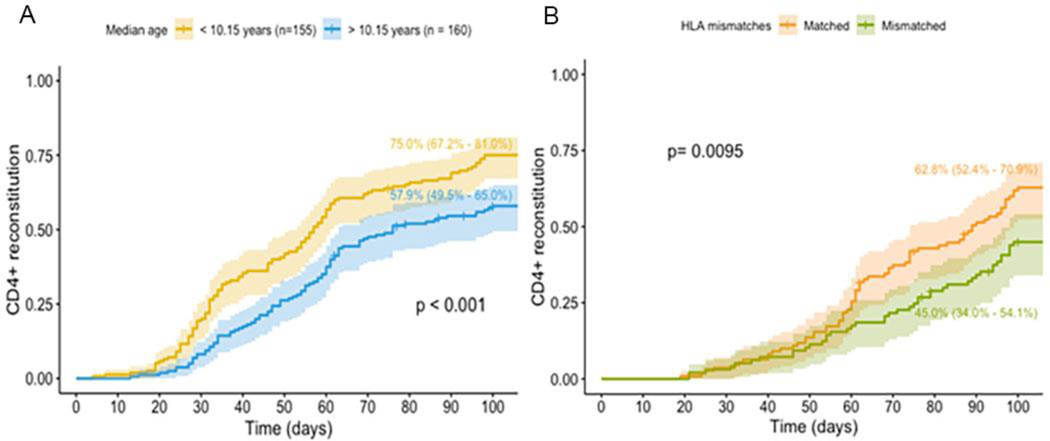
Results: In this analysis, 315 patients with a median age of 10.4 years (interquartile range 5.0-16.5 years) were included. The cumulative incidence of CD4+ IR at 100 days was 66.7% in the entire cohort, 54.7% in TCD (N = 208, hazard ratio [HR] 0.47, P < 0.001), 90.0% in uCB (N = 40) and 89.6% in T-replete (N = 47) HCT recipients. In multi-variate analyses, not achieving early CD4+ IR was a predictor of inferior OS (HR 2.35, 95% confidence interval [CI] 1.46-3.79, P < 0.001) and EFS (HR 1.80, 95% CI 1.20-2.69, P = 0.004) and increased NRM (HR 6.58, 95% CI 2.82-15.38, P < 0.001). No impact of CD4+ IR on relapse or aGVHD was found. Within the TCD group, similar associations were observed.
Conclusion: In this HCT cohort, including recipients of TCD HCT, we confirmed that early CD4+ IR was an excellent predictor of outcomes. Finding strategies to predict or improve CD4+ IR may influence outcomes.
Keywords: CD4 T Cells; Hematopoietic transplant; Pediatric; T-cell reconstitution; immune reconstitution.
Copyright © 2020 International Society for Cell and Gene Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Savani BN, Mielke S, Rezvani K, Montero A, Yong AS, Wish L, Superata J, Kurlander R, Singh A, Childs R, Barrett AJ, Absolute lymphocyte count on day 30 is a surrogate for robust hematopoietic recovery and strongly predicts outcome after T cell-depleted allogeneic stem cell transplantation, Biol Blood Marrow Transplant 13(10) (2007) 1216–23. - PMC - PubMed
-
- Admiraal R, de Koning CCH, Lindemans CA, Bierings MB, Wensing AMJ, Versluys AB, Wolfs TFW, Nierkens S, Boelens JJ, Viral reactivations and associated outcomes in the context of immune reconstitution after pediatric hematopoietic cell transplantation, J Allergy Clin Immunol 140(6) (2017) 1643–1650 e9. - PubMed
-
- Berger M, Figari O, Bruno B, Raiola A, Dominietto A, Fiorone M, Podesta M, Tedone E, Pozzi S, Fagioli F, Madon E, Bacigalupo A, Lymphocyte subsets recovery following allogeneic bone marrow transplantation (BMT): CD4+ cell count and transplant-related mortality, Bone Marrow Transplant 41(1) (2008) 55–62. - PubMed
-
- Fedele R, Martino M, Garreffa C, Messina G, Console G, Princi D, Dattola A, Moscato T, Massara E, Spiniello E, Irrera G, Iacopino P, The impact of early CD4+ lymphocyte recovery on the outcome of patients who undergo allogeneic bone marrow or peripheral blood stem cell transplantation, Blood Transfus 10(2) (2012) 174–80. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
