

Coronavirus disease (COVID-19) and the liver: a comprehensive systematic review and meta-analysis
- PMID: 32623633
- PMCID: PMC7335221
- DOI: 10.1007/s12072-020-10071-9
Coronavirus disease (COVID-19) and the liver: a comprehensive systematic review and meta-analysis
Abstract
Background: Liver function derangements have been reported in coronavirus disease (COVID-19), but reported rates are variable.
Methods: We searched PubMed and Embase with terms COVID and SARS-COV-2 from December 1, 2019 till April 5, 2020. We estimated overall prevalence, stratified prevalence based on severity, estimated risk ratio (RR), and estimated standardized mean difference (SMD) of liver function parameters in severe as compared to non-severe COVID. Random effect method utilizing inverse variance approach was used for pooling the data.
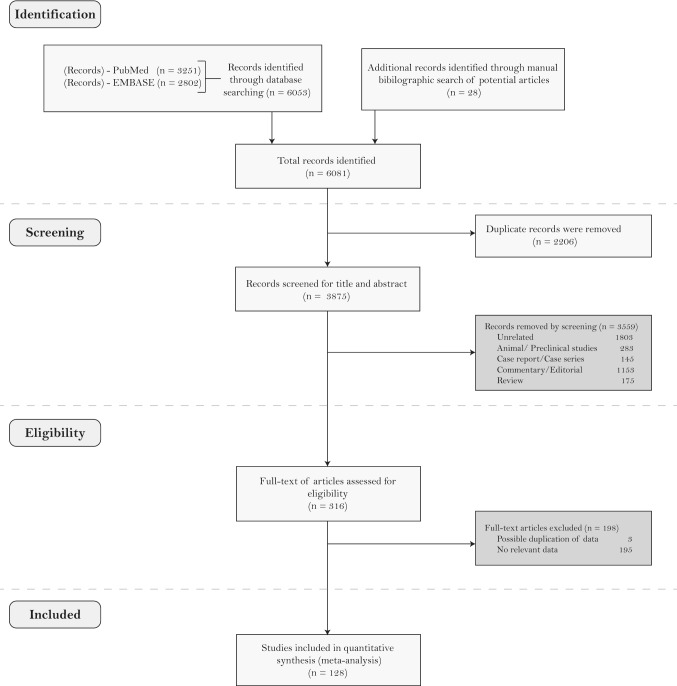
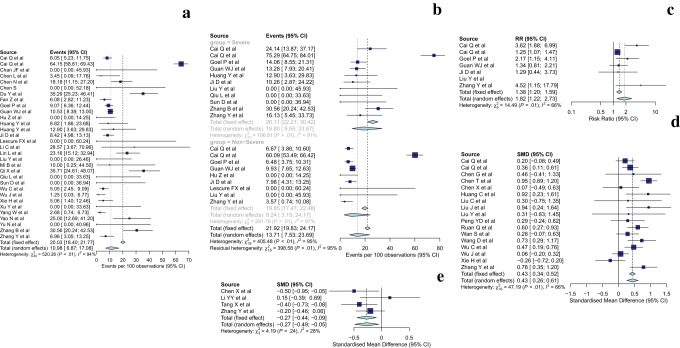
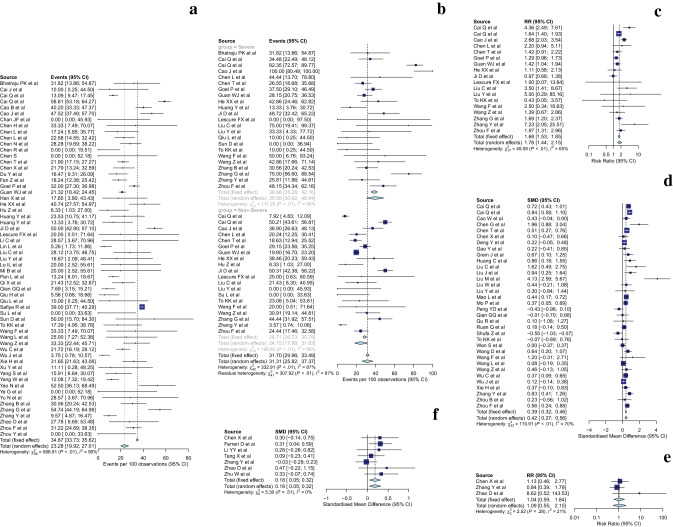
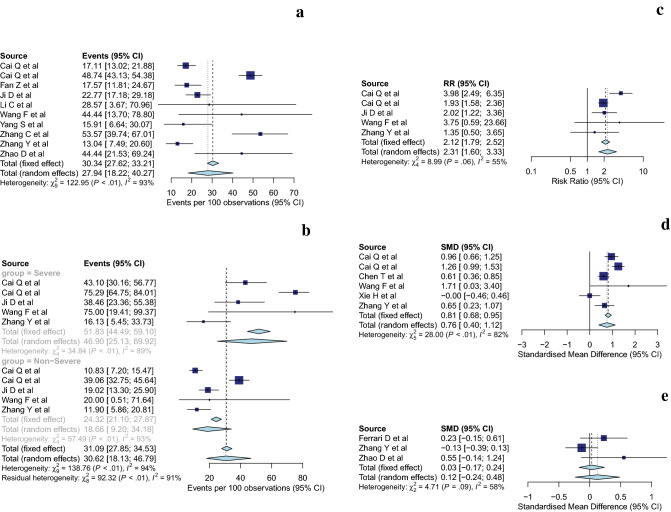
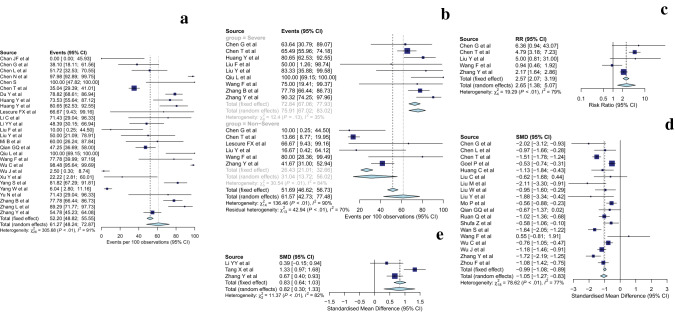
Results: In all, 128 studies were included. The most frequent abnormalities were hypoalbuminemia [61.27% (48.24-72.87)], elevations of gamma-glutamyl transferase (GGT) [27.94% (18.22-40.27)], alanine aminotransferase (ALT) [23.28% (19.92-27.01)], and aspartate aminotransferase (AST) [23.41% (18.84-28.70)]. Furthermore, the relative risk of these abnormalities was higher in the patients with severe COVID-19 when compared to non-severe disease [Hypoalbuminemia-2.65 (1.38-5.07); GGT-2.31 (1.6-3.33); ALT-1.76 (1.44-2.15); AST-2.30 (1.82-2.90)]. The SMD of hypoalbuminemia, GGT, ALT, and AST elevation in severe as compared to non-severe were - 1.05 (- 1.27 to - 0.83), 0.76 (0.40-1.12), 0.42 (0.27-0.56), and 0.69 (0.52-0.86), respectively. The pooled prevalence and RR of chronic liver disease as a comorbidity was 2.64% (1.73-4) and 1.69 (1.05-2.73) respectively.
Conclusion: The most frequent abnormality in liver functions was hypoalbuminemia followed by derangements in gamma-glutamyl transferase and aminotransferases, and these abnormalities were more frequent in severe disease. The systematic review was, however, limited by heterogeneity in definitions of severity and liver function derangements. Graphical depiction of the summary of meta-analytic findings a) pooled prevalence of abnormalities b) Risk ratio of abnormality in severe versus non-severe COVID-19 c) standardized mean difference (SMD) between severe and non-severe group and d) pooled prevalence for parameters based on severity stratification for bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), albumin, globulin and acute hepatic injury (AHI) . Also estimates for overall/total liver disease (TLD) and chronic liver disease (CLD) amongst COVID-19 patients are depicted in a, b, d. For d) In addition to severity stratification, Overall (all studies for a particular estimate) and combined (only those studies which reported severity) estimates are provided.
Keywords: COVID-19; Cirrhosis; Histology; SARS-CoV-2; Transplantation.
Conflict of interest statement
M. Praveen Kumar, Shubhra Mishra, Daya Krishna Jha, Jayendra Shukla, Arup Choudhury, Ritin Mohindra, Harshal S. Mandavdhare, Usha Dutta, and Vishal Sharma declare that they have no conflict of interest.
Figures
References
-
- World Health Organisation. Interim guidance: Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected. 2nd Edition. WHO/2019-nCoV/clinical/2020.4
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
