

The rapid transformation of cardiac surgery practice in the coronavirus disease 2019 (COVID-19) pandemic: Insights and clinical strategies from a center at the epicenter
- PMID: 32624303
- PMCID: PMC7331531
- DOI: 10.1016/j.jtcvs.2020.04.060
The rapid transformation of cardiac surgery practice in the coronavirus disease 2019 (COVID-19) pandemic: Insights and clinical strategies from a center at the epicenter
Abstract
Background: The onset of the coronavirus disease 2019 (COVID-19) pandemic has forced our cardiac surgery program and hospital to enact drastic measures that has forced us to change how we care for cardiac surgery patients, assist with COVID-19 care, and enable support for the hospital in terms of physical resources, providers, and resident training.
Methods: In this review, we review the cardiovascular manifestations of COVID-19 and describe our system-wide adaptations to the pandemic, including the use of telemedicine, how a severe reduction in operative volume affected our program, the process of redeployment of staff, repurposing of residents into specific task teams, the creation of operation room intensive care units, and the challenges that we faced in this process.
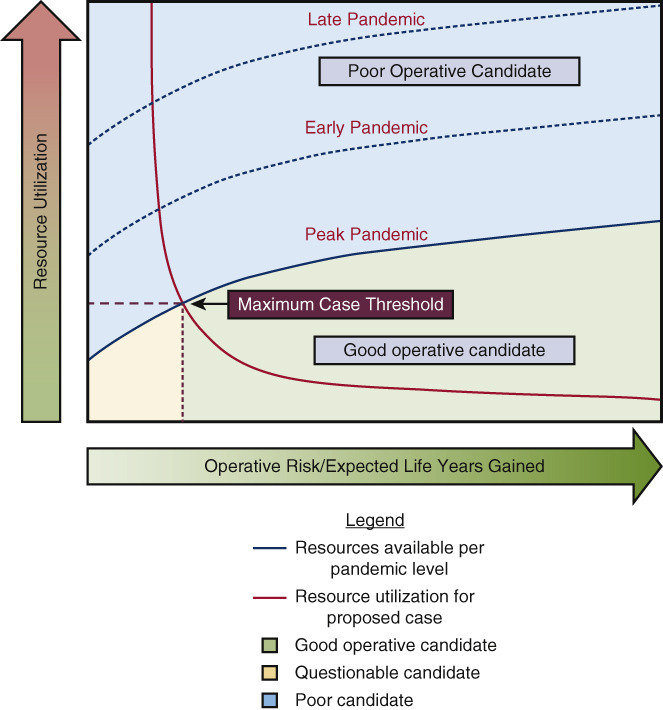
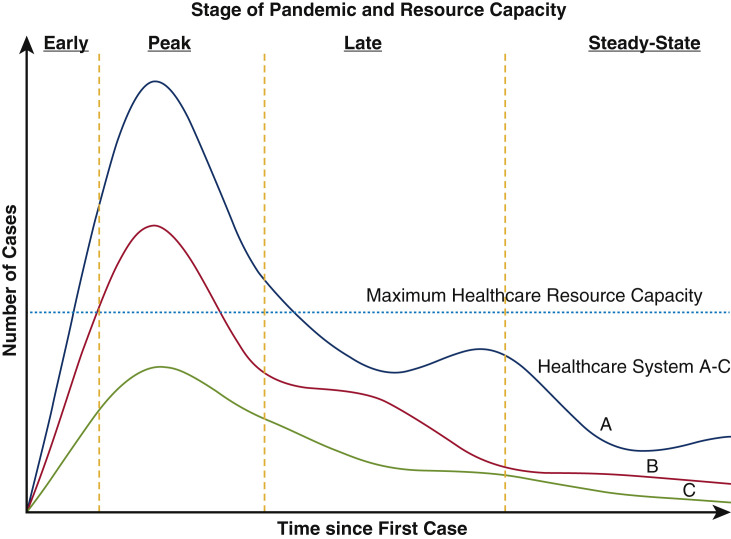
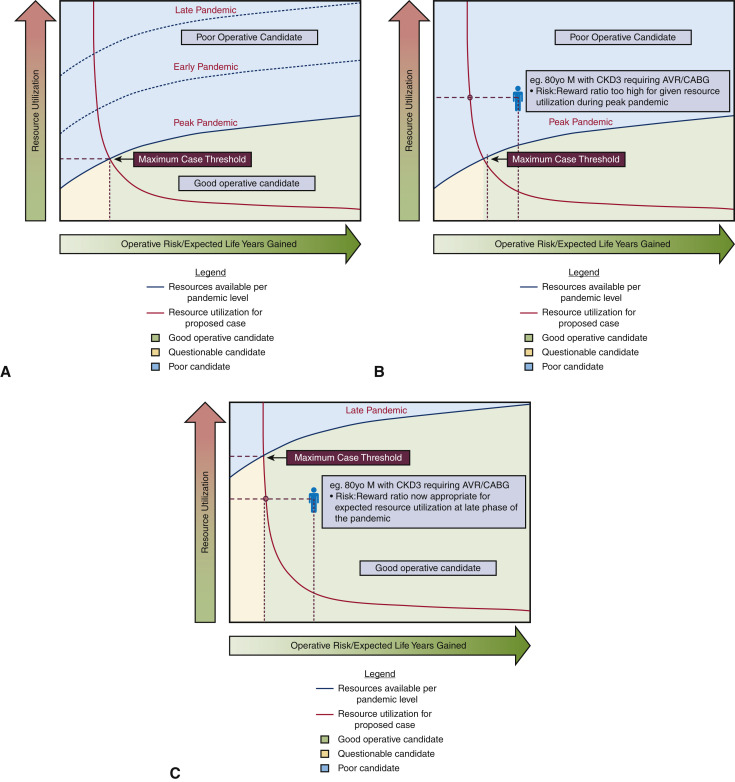
Results: We offer a revised set of definitions of surgical priority during this pandemic and how this was applied to our system, followed by specific considerations in coronary/valve, aortic, heart failure and transplant surgery. Finally, we outline a path forward for cardiac surgery for the near future.
Conclusions: We recognize that individual programs around the world will eventually face COVID-19 with varying levels of infection burden and different resources, and we hope this document can assist programs to plan for the future.
Keywords: COVID-19; New York; cardiac surgery; pandemic; reorganization.
Copyright © 2020 Jointly between The American Association for Thoracic Surgery, The Society of Thoracic Surgeons, and the European Association for Cardio-Thoracic Surgery. Published by Elsevier Inc. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Commentary: Implications of coronavirus disease 2019 (COVID-19) for cardiac surgery: Priorities and decisions.J Thorac Cardiovasc Surg. 2020 Oct;160(4):951-952. doi: 10.1016/j.jtcvs.2020.05.064. Epub 2020 Jun 4. J Thorac Cardiovasc Surg. 2020. PMID: 32605729 Free PMC article. No abstract available.
-
Commentary: Pandemic deployment and surgical soldiership.J Thorac Cardiovasc Surg. 2020 Oct;160(4):952-953. doi: 10.1016/j.jtcvs.2020.05.059. Epub 2020 Jun 5. J Thorac Cardiovasc Surg. 2020. PMID: 32622576 Free PMC article. No abstract available.
-
Commentary: Vulnerability and resilience demonstrated: Cardiac surgeons during coronavirus disease 2019 (COVID-19).J Thorac Cardiovasc Surg. 2020 Oct;160(4):949-950. doi: 10.1016/j.jtcvs.2020.05.068. Epub 2020 Jun 4. J Thorac Cardiovasc Surg. 2020. PMID: 32651004 Free PMC article. No abstract available.
-
Commentary: Preparation for pandemics prevents pandemonium.J Thorac Cardiovasc Surg. 2020 Oct;160(4):948-949. doi: 10.1016/j.jtcvs.2020.05.067. Epub 2020 Jun 6. J Thorac Cardiovasc Surg. 2020. PMID: 32763042 Free PMC article. No abstract available.
References
-
- Johns Hopkins University Coronavirus Resource Center COVID-19 Dashboard by the Center for Systems Science and Engineering at Johns Hopkins University. 2020. https://coronavirus.jhu.edu/map.html Available at: Accessed April 6, 2020.
-
- Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. J Am Med Assoc. 2020;323:1239–1242. - PubMed
-
- Bonow R.O., Fonarow G.C., O'Gara P.T., Yancy C.W. Association of coronavirus disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. March 27, 2020 [Epub ahead of print] - PubMed
-
- Guo J., Huang Z., Lin L., Lv J. Coronavirus disease 2019 (COVID-19) and cardiovascular disease: a viewpoint on the potential influence of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers on onset and severity of severe acute respiratory syndrome coronavirus 2 infection. J Am Heart Assoc. 2020;9:e016219. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
