

COVID-19 infection and diffusion among the healthcare workforce in a large university-hospital in northwest Italy
- PMID: 32624560
- PMCID: PMC7809947
- DOI: 10.23749/mdl.v111i3.9767
COVID-19 infection and diffusion among the healthcare workforce in a large university-hospital in northwest Italy
Abstract
Backgroud: Since the beginning of the coronavirus disease 2019 (COVID-19) outbreak, healthcare workers (HCWs) have been the workers most likely to contract the disease. Intensive focus is therefore needed on hospital strategies that minimize exposure and diffusion, confer protection and facilitate early detection and isolation of infected personnel.
Methods: To evaluate the early impact of a structured risk-management for exposed COVID-19 HCWs and describe how their characteristics contributed to infection and diffusion. Socio-demographic and clinical data, aspects of the event-exposure (date, place, length and distance of exposure, use of PPE) and details of the contact person were collected.
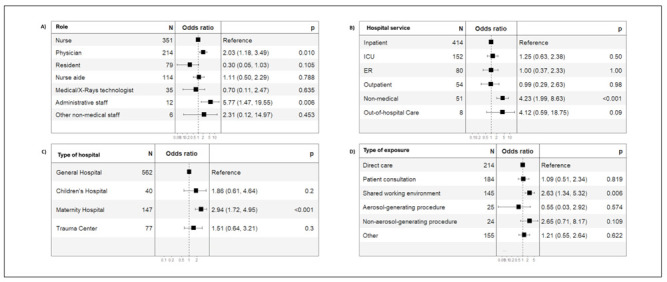
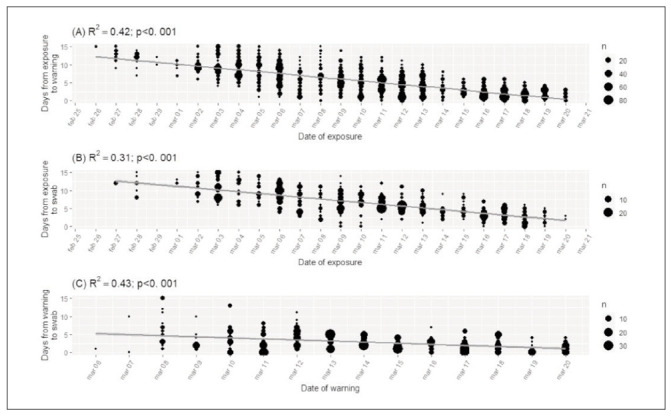
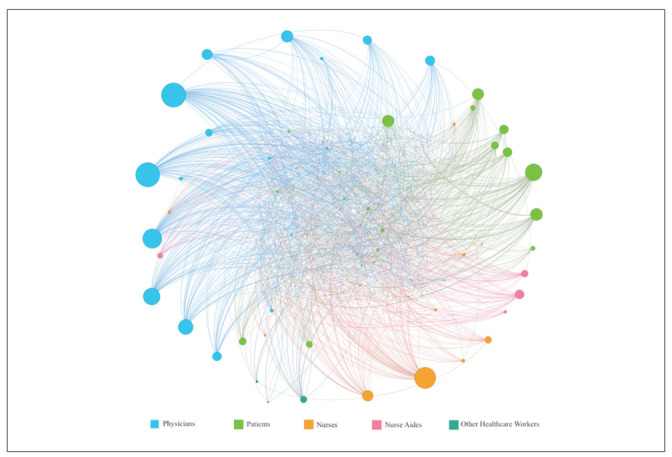
Results: The 2411 HCWs reported 2924 COVID-19 contacts. Among 830 HCWs who were at 'high or medium risk', 80 tested positive (9.6%). Physicians (OR=2.03), and non-medical services -resulted in an increased risk (OR=4.23). Patient care did not increase the risk but sharing the work environment did (OR=2.63). There was a significant time reduction between exposure and warning, exposure and test, and warning and test since protocol implementation. HCWs with management postitions were the main source of infection due to the high number of interactions.
Discussion: A proactive system that includes prompt detection of contagious staff and identification of sources of exposure helps to lower the intra-hospital spread of infection. A speedier return to work of staff who would otherwise have had to self-isolate as a precautionary measure improves staff morale and patient care by reducing the stress imposed by excessive workloads arising from staff shortages.
«Come l’infezione da COVID-19 si è diffusa tra i lavoratori di un grande ospedale universitario nel nord-ovest Italia»
Introduzione:: Fin dall’inizio dell’epidemia di Coronavirus-2019 (COVID-19), gli operatori sanitari (HCW) sono stati i lavoratori che hanno avuto maggiori probabilità di contrarre la malattia. È pertanto necessario un focus sulle strategie ospedaliere per ridurre al minimo l’esposizione e la diffusione dell’infezione, e che possano facilitare l’individuazione precoce e l’isolamento del personale infetto.
Metodi:: Valutare l’impatto iniziale di una gestione strutturata del rischio per gli HCW esposti a COVID-19 e descrivere come le loro caratteristiche hanno contribuito all’infezione e alla sua diffusione. Sono stati raccolti dati socio-demografici e clinici, aspetti dell’esposizione (data, luogo, lunghezza e distanza dell’esposizione, uso dei DPI) e dettagli della persona fonte.
Risultati:: 2411 operatori sanitari hanno riportato 2924 contatti COVID-19. Tra gli 830 operatori sanitari a rischio alto o medio, 80 sono risultati positivi (9,6%). I medici (OR = 2,03) e i servizi non medici hanno comportato un aumento del rischio (OR=4,23). L’assistenza ai pazienti non ha aumentato il rischio, ma una condivisione dell’ambiente di lavoro (OR=2,63). Vi è stata una significativa riduzione del tempo tra esposizione e segnalazione, esposizione e test e segnalazione e test dall’implementazione del protocollo. Gli operatori sanitari con ruolo di coordinamento è stata la principale fonte di infezione a causa dell’elevato numero di interazioni all’inizio dell’epidemia.
Discussione:: Un sistema proattivo che includa la rilevazione tempestiva del personale contagioso e l’identificazione delle fonti di esposizione aiuta a ridurre la diffusione dell’infezione all’interno dell’ospedale. Un rapido ritorno al lavoro dei lavoratori, che altrimenti avrebbero dovuto autoisolarsi come misura precauzionale, migliora la cura dei pazienti riducendo lo stress imposto da carichi di lavoro eccessivi derivanti dalla carenza di personale.
Figures
References
-
- Adams JG, Walls RM. Supporting the health care workforce during the COVID-19 global epidemic. JAMA. (Published online March 12, 2020) doi:10.1001/jama.2020.3972. - PubMed
-
- Bastian M, Heymann S, Jacomy M. (2009). Gephi: an open source software for exploring and manipulating networks. Available on line at: https://gephi.org/publications/gephi-bastian-feb09.pdf. (last accessed 09-04-2020)
-
- Blondel VD, Guillaume JL, Lambiotte R. Lefebvre: Fast unfolding of communities in large networks. J Stat Mech. 2008;10:P10008.
-
- CDC, Centers for Disease Control and Prevention. (2020). Interim guidelines for collecting, handling, and testing clinical specimens from persons for coronavirus disease 2019 (COVID-19) Available on line at: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specim.... (last accessed 09-04-2020)
