

Invasive Lobular Breast Carcinoma Can Be a Challenging Diagnosis Without the Use of Tumor Markers
- PMID: 32626620
- PMCID: PMC7328694
- DOI: 10.7759/cureus.8376
Invasive Lobular Breast Carcinoma Can Be a Challenging Diagnosis Without the Use of Tumor Markers
Abstract
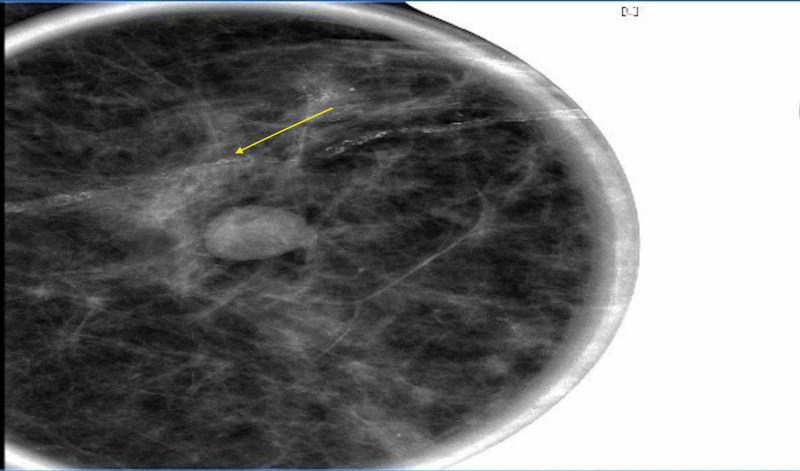
Invasive lobular carcinoma is often challenging to diagnose due to the lack of physical examination findings and macrocalcifications on mammography. The cells of invasive lobular carcinoma form a distinct single file pattern that can be identified on histology slides. Often, when patients present, there is metastasis to the bones, lymph nodes, and gastrointestinal tract. Tumor markers are a valuable tool in identification, especially the loss of E-cadherin protein. However, if E-cadherin protein is not available, epidermal membrane antigen, which inhibits E-cadherin, can prove to be a significant diagnostic tool. Epidermal membrane antigen was the key tumor marker in our patient case. Other tumor markers and histology stains can drive treatment plans and help predict prognosis.
Keywords: cam 5.2; e-cadherin; er positive; hematoxylin and eosin; her 2 negative; invasive lobular carcinoma; mammogram; metastatic breast cancer; single-file pattern; tumor markers.
Copyright © 2020, Klumpp et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures







References
-
- Metastatic lobular carcinoma of the breast: patterns of spread in the chest, abdomen, and pelvis on CT. Winston CB, Hadar O, Teitcher JB, Caravelli JF, Sklarin NT, Panicek DM, Liberman L. AJR Am J Roentgenol. 2000;175:795–800. - PubMed
-
- Breast Cancer—Health Professional Version. [May;2020 ];https://www.cancer.gov/types/breast/hp 2020
-
- Lobular breast cancer: molecular basis, mouse and cellular models. Christgen M, Derksen P. http://10.1186/s13058-015-0517-z. Breast Cancer Res. 2015;17:16. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials