

In-vitro diagnostic point-of-care tests in paediatric ambulatory care: A systematic review and meta-analysis
- PMID: 32628707
- PMCID: PMC7337322
- DOI: 10.1371/journal.pone.0235605
In-vitro diagnostic point-of-care tests in paediatric ambulatory care: A systematic review and meta-analysis
Abstract
Introduction: Paediatric consultations form a significant proportion of all consultations in ambulatory care. Point-of-care tests (POCTs) may offer a potential solution to improve clinical outcomes for children by reducing diagnostic uncertainty in acute illness, and streamlining management of chronic diseases. However, their clinical impact in paediatric ambulatory care is unknown. We aimed to describe the clinical impact of all in-vitro diagnostic POCTs on patient outcomes and healthcare processes in paediatric ambulatory care.
Methods: We searched MEDLINE, EMBASE, Pubmed, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and Web of Science from inception to 29 January 2020 without language restrictions. We included studies of children presenting to ambulatory care settings (general practice, hospital outpatient clinics, or emergency departments, walk-in centres, registered drug shops delivering healthcare) where in-vitro diagnostic POCTs were compared to usual care. We included all quantitative clinical outcome data across all conditions or infection syndromes reporting on the impact of POCTs on clinical care and healthcare processes. Where feasible, we calculated risk ratios (RR) with 95% confidence intervals (CI) by performing meta-analysis using random effects models.
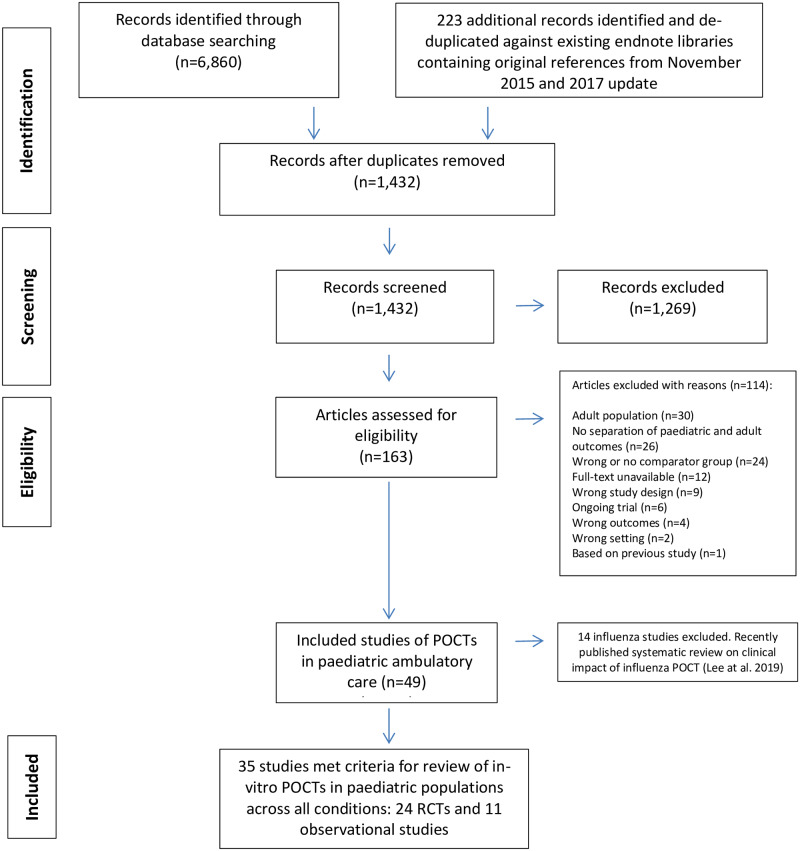
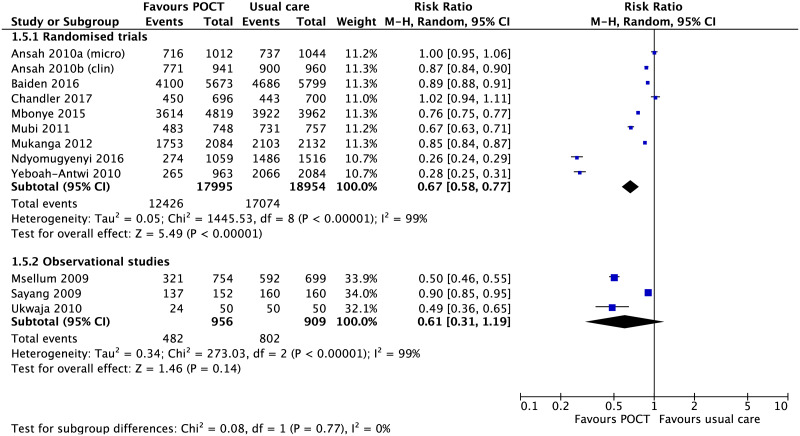
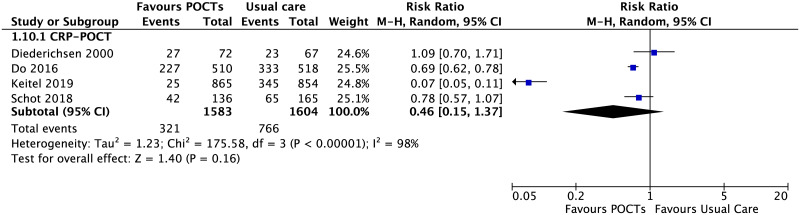
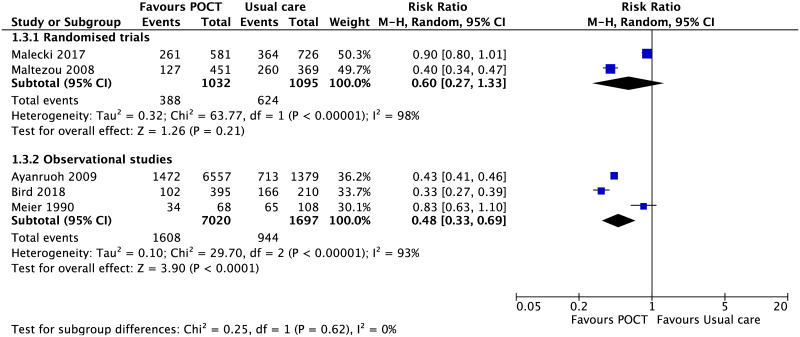
Results: We included 35 studies. Data relating to at least one outcome were available for 89,439 children of whom 45,283 had a POCT across six conditions or infection syndromes: malaria (n = 14); non-specific acute fever 'illness' (n = 7); sore throat (n = 5); acute respiratory tract infections (n = 5); HIV (n = 3); and diabetes (n = 1). Outcomes centred around decision-making such as prescription of medications or hospital referral. Pooled estimates showed that malarial-POCTs (Plasmodium falciparum) better targeted antimalarial treatment by reducing over-treatment by a third compared to usual care (RR 0.67; 95% CI [0.58 to 0.77], n = 36,949). HIV-POCTs improved initiating earlier antiretroviral therapy compared to usual care (RR, 3.11; 95% CI [1.55 to 6.25], n = 912). Across the other four conditions, there was limited evidence for the benefit of POCTs in paediatric ambulatory care except for acute respiratory tract infections (RTI) in low-and-middle-income countries (LMICs), where POCT C-Reactive Protein (CRP) may reduce immediate antibiotic prescribing by a third (risk difference, -0.29 [-0.47, -0.11], n = 2,747). This difference was shown in randomised controlled trials in LMICs which included guidance on interpretation of POCT-CRP, specific training or employed a diagnostic algorithm prior to POC testing.
Conclusion: Overall, there is a paucity of evidence for the use of POCTs in paediatric ambulatory care. POCTs help to target prescribing for children with malaria and HIV. There is emerging evidence that POCT-CRP may better target antibiotic prescribing for children with acute RTIs in LMIC, but not in high-income countries. Research is urgently needed to understand where POCTs are likely to improve clinical outcomes in paediatric settings worldwide.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Evidence review for rapid tests to inform triage and antibiotic prescribing decisions: Suspected acute respiratory infection in over 16s: assessment at first presentation and initial management: Evidence review B.London: National Institute for Health and Care Excellence (NICE); 2023 Oct. London: National Institute for Health and Care Excellence (NICE); 2023 Oct. PMID: 38170807 Free Books & Documents. Review.
-
C-reactive protein point-of-care testing for safely reducing antibiotics for acute exacerbations of chronic obstructive pulmonary disease: the PACE RCT.Health Technol Assess. 2020 Mar;24(15):1-108. doi: 10.3310/hta24150. Health Technol Assess. 2020. PMID: 32202490 Free PMC article. Clinical Trial.
-
Impact of point-of-care C reactive protein in ambulatory care: a systematic review and meta-analysis.BMJ Open. 2019 Feb 1;9(1):e025036. doi: 10.1136/bmjopen-2018-025036. BMJ Open. 2019. PMID: 30782747 Free PMC article.
-
Impact of point-of-care panel tests in ambulatory care: a systematic review and meta-analysis.BMJ Open. 2020 Feb 27;10(2):e032132. doi: 10.1136/bmjopen-2019-032132. BMJ Open. 2020. PMID: 32111610 Free PMC article.
Cited by
-
Be-SNAP: the Belgian Sepsis National Action Plan.Front Public Health. 2025 Jul 1;13:1575502. doi: 10.3389/fpubh.2025.1575502. eCollection 2025. Front Public Health. 2025. PMID: 40666145 Free PMC article.
-
Impact of educational training and C-reactive protein point-of-care testing on antibiotic prescribing in rural and urban family physician practices in Latvia: a randomised controlled intervention study.BMC Pediatr. 2022 Sep 21;22(1):556. doi: 10.1186/s12887-022-03608-4. BMC Pediatr. 2022. PMID: 36127630 Free PMC article. Clinical Trial.
-
Biomarkers as point-of-care tests to guide prescription of antibiotics in people with acute respiratory infections in primary care.Cochrane Database Syst Rev. 2022 Oct 17;10(10):CD010130. doi: 10.1002/14651858.CD010130.pub3. Cochrane Database Syst Rev. 2022. PMID: 36250577 Free PMC article.
-
Adoption of C-reactive protein rapid tests for the management of acute childhood infections in hospitals in the Netherlands and England: a comparative health systems analysis.BMC Health Serv Res. 2024 Mar 19;24(1):351. doi: 10.1186/s12913-024-10698-6. BMC Health Serv Res. 2024. PMID: 38504318 Free PMC article.
-
Neutrophil gelatinase-associated lipocalin is elevated in children with acute kidney injury and sickle cell anemia, and predicts mortality.Kidney Int. 2022 Oct;102(4):885-893. doi: 10.1016/j.kint.2022.05.020. Epub 2022 Jun 17. Kidney Int. 2022. PMID: 35718113 Free PMC article.
References
-
- O’Neill J. Tackling Drug-Resistant Infections Globally: final report and recommendations. 2016.
-
- Aabenhus R, Jensen JU, Jorgensen KJ, Hrobjartsson A, Bjerrum L. Biomarkers as point-of-care tests to guide prescription of antibiotics in patients with acute respiratory infections in primary care. The Cochrane database of systematic reviews. 2014(11):Cd010130 10.1002/14651858.CD010130.pub2 - DOI - PubMed
-
- Little P, Stuart B, Francis N, Douglas E, Tonkin-Crine S, Anthierens S, et al. Effects of internet-based training on antibiotic prescribing rates for acute respiratory-tract infections: a multinational, cluster, randomised, factorial, controlled trial. Lancet (London, England). 2013;382(9899):1175–82. - PMC - PubMed
-
- Althaus T, Greer RC, Swe MMM, Cohen J, Tun NN, Heaton J, et al. Effect of point-of-care C-reactive protein testing on antibiotic prescription in febrile patients attending primary care in Thailand and Myanmar: an open-label, randomised, controlled trial. The Lancet Global health. 2019;7(1):e119–e31. 10.1016/S2214-109X(18)30444-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
