

Mobility restrictions for the control of epidemics: When do they work?
- PMID: 32628716
- PMCID: PMC7337314
- DOI: 10.1371/journal.pone.0235731
Mobility restrictions for the control of epidemics: When do they work?
Abstract
Background: Mobility restrictions-trade and travel bans, border closures and, in extreme cases, area quarantines or cordons sanitaires-are among the most widely used measures to control infectious diseases. Restrictions of this kind were important in the response to epidemics of SARS (2003), H1N1 influenza (2009), Ebola (2014) and, currently in the containment of the ongoing COVID-19 pandemic. However, they do not always work as expected.
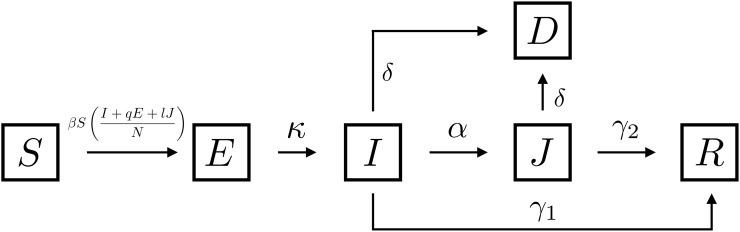
Methods: To determine when mobility restrictions reduce the size of an epidemic, we use a model of disease transmission within and between economically heterogeneous locally connected communities. One community comprises a low-risk, low-density population with access to effective medical resources. The other comprises a high-risk, high-density population without access to effective medical resources.
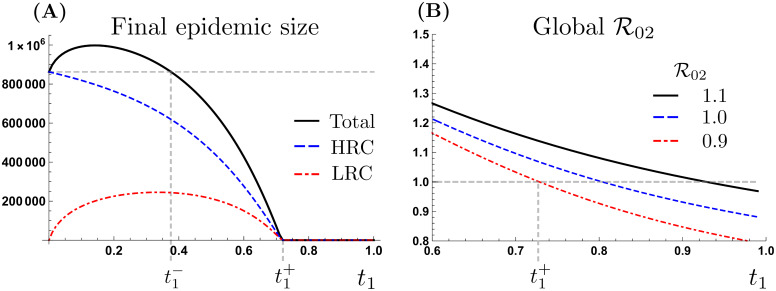
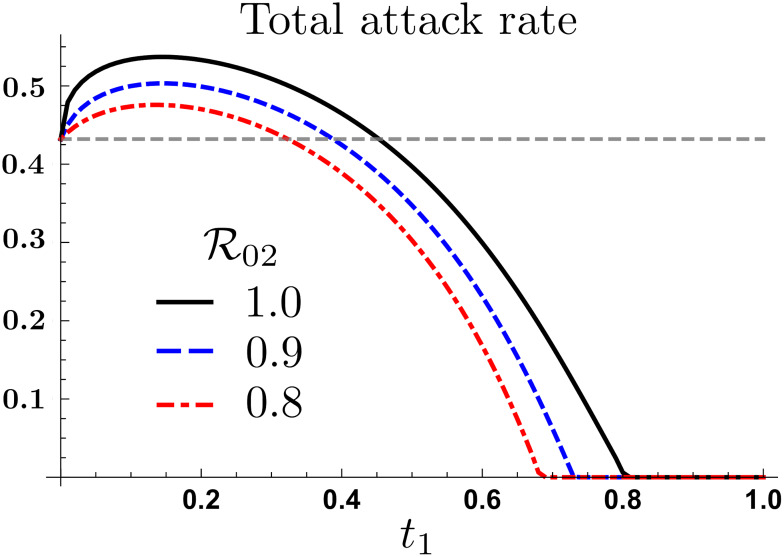
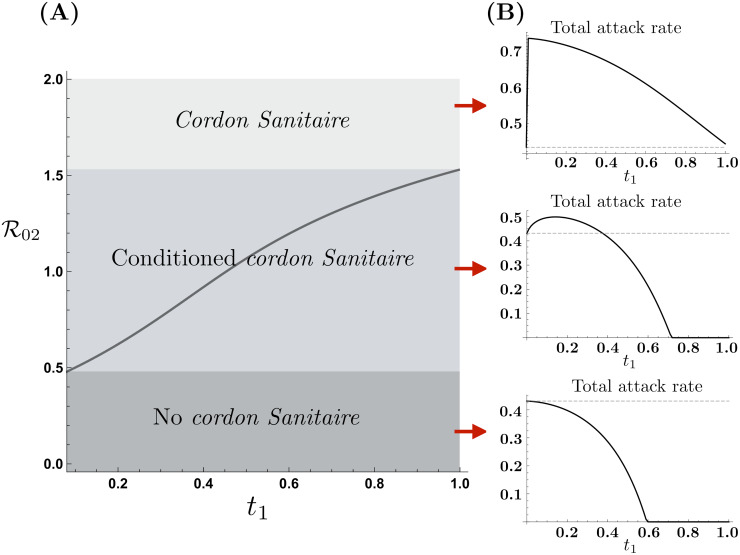
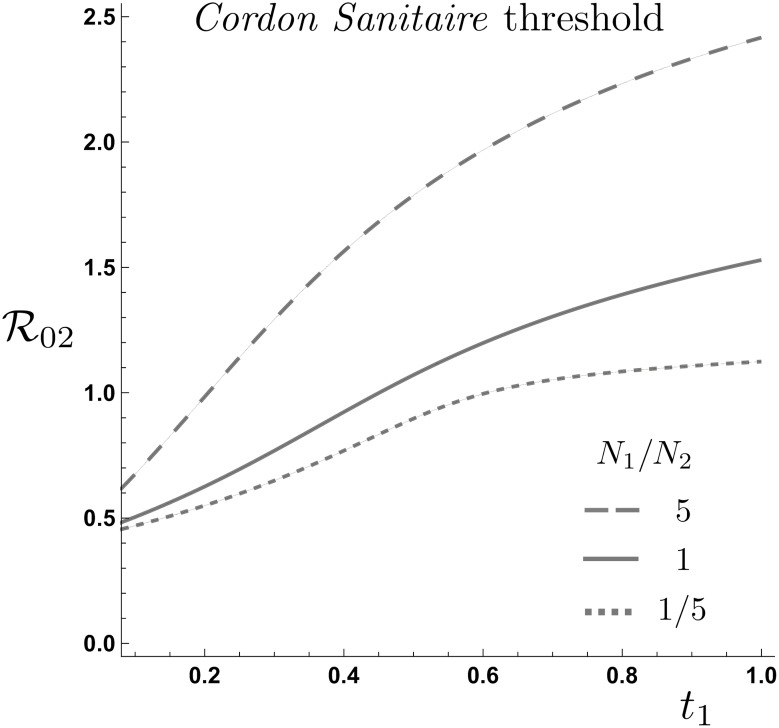
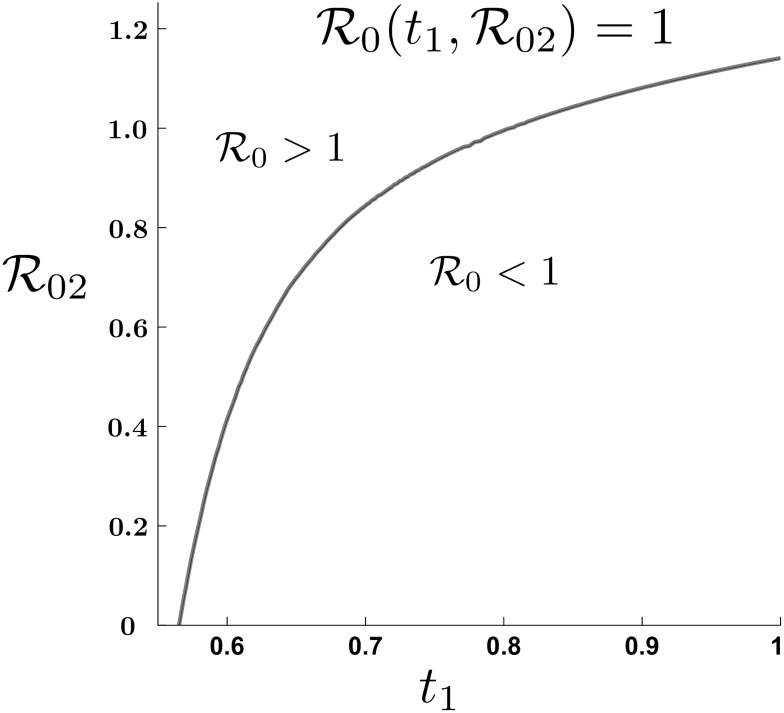
Findings: Unrestricted mobility between the two risk communities increases the number of secondary cases in the low-risk community but reduces the overall epidemic size. By contrast, the imposition of a cordon sanitaire around the high-risk community reduces the number of secondary infections in the low-risk community but increases the overall epidemic size.
Interpretation: Mobility restrictions may not be an effective policy for controlling the spread of an infectious disease if it is assessed by the overall final epidemic size. Patterns of mobility established through the independent mobility and trade decisions of people in both communities may be sufficient to contain epidemics.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Race P. Some further consideration of the plague in Eyam, 1665/6. Local population studies. 1995;54:56–57. - PubMed
-
- Arnebeck B. A short history of yellow fever in the US. Bob Arnebeck. 2008.
-
- Kohn GC. Encyclopedia of plague and pestilence: from ancient times to the present. Infobase Publishing; 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
