

Is mammography screening beneficial: An individual-based stochastic model for breast cancer incidence and mortality
- PMID: 32628726
- PMCID: PMC7365474
- DOI: 10.1371/journal.pcbi.1008036
Is mammography screening beneficial: An individual-based stochastic model for breast cancer incidence and mortality
Abstract
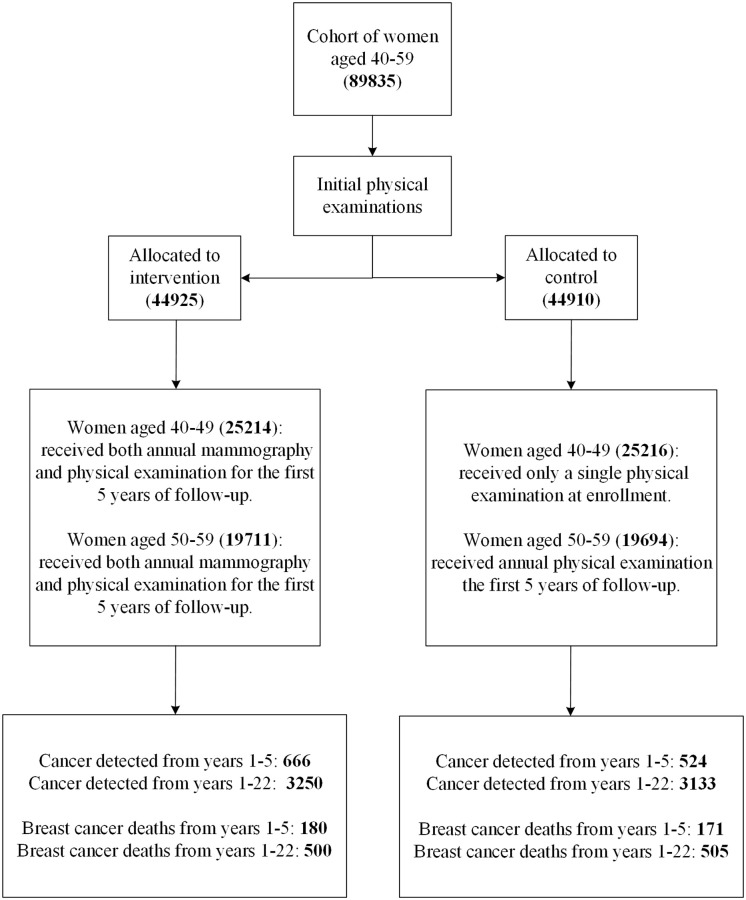
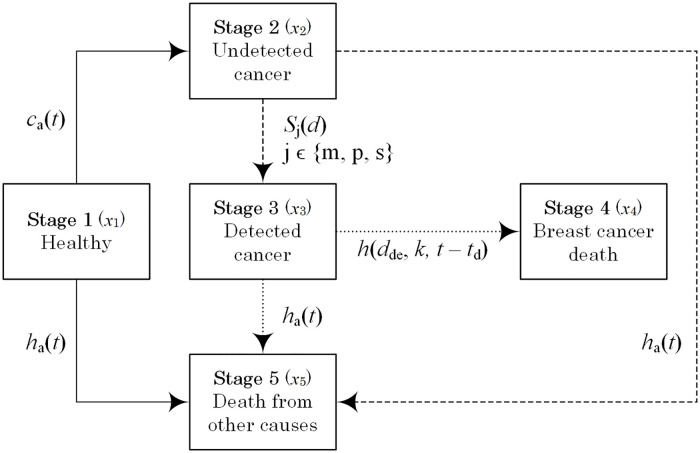
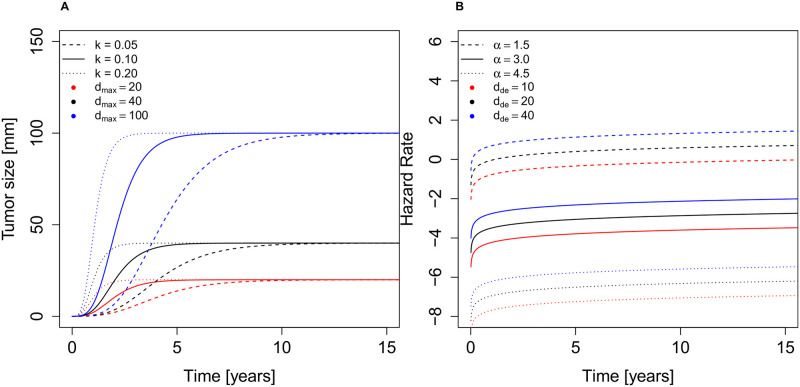
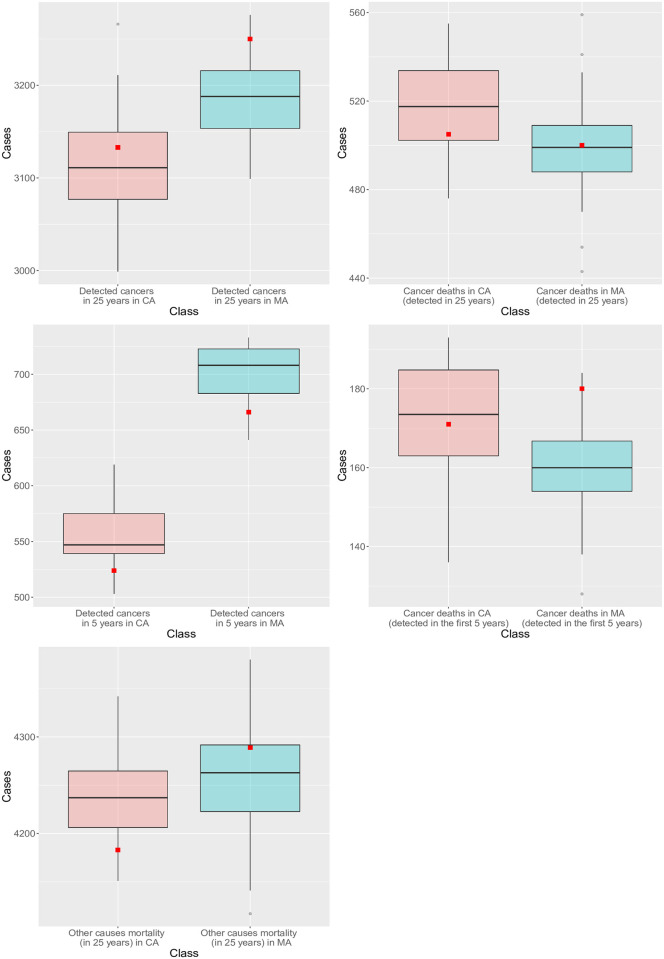
The benefits of mammography screening have been controversial, with conflicting findings from various studies. We hypothesize that unmeasured heterogeneity in tumor aggressiveness underlies these conflicting results. Based on published data from the Canadian National Breast Screening Study (CNBSS), we develop and parameterize an individual-based mechanistic model for breast cancer incidence and mortality that tracks five stages of breast cancer progression and incorporates the effects of age on breast cancer incidence and all-cause mortality. The model accurately reproduces the reported outcomes of the CNBSS. By varying parameters, we predict that the benefits of mammography depend on the effectiveness of cancer treatment and tumor aggressiveness. In particular, patients with the most rapidly growing or potentially largest tumors have the highest benefit and least harm from the screening, with only a relatively small effect of age. However, the model predicts that confining mammography to populations with a high risk of acquiring breast cancer increases the screening benefit only slightly compared with the full population.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
