

A Multi-atlas Approach for Active Bone Marrow Sparing Radiation Therapy: Implementation in the NRG-GY006 Trial
- PMID: 32629079
- PMCID: PMC7944643
- DOI: 10.1016/j.ijrobp.2020.06.071
A Multi-atlas Approach for Active Bone Marrow Sparing Radiation Therapy: Implementation in the NRG-GY006 Trial
Abstract
Purpose: Sparing active bone marrow (ABM) can reduce acute hematologic toxicity in patients undergoing chemoradiotherapy for cervical cancer, but ABM segmentation based on positron emission tomography/computed tomography (PET/CT) is costly. We sought to develop an atlas-based ABM segmentation method for implementation in a prospective clinical trial.
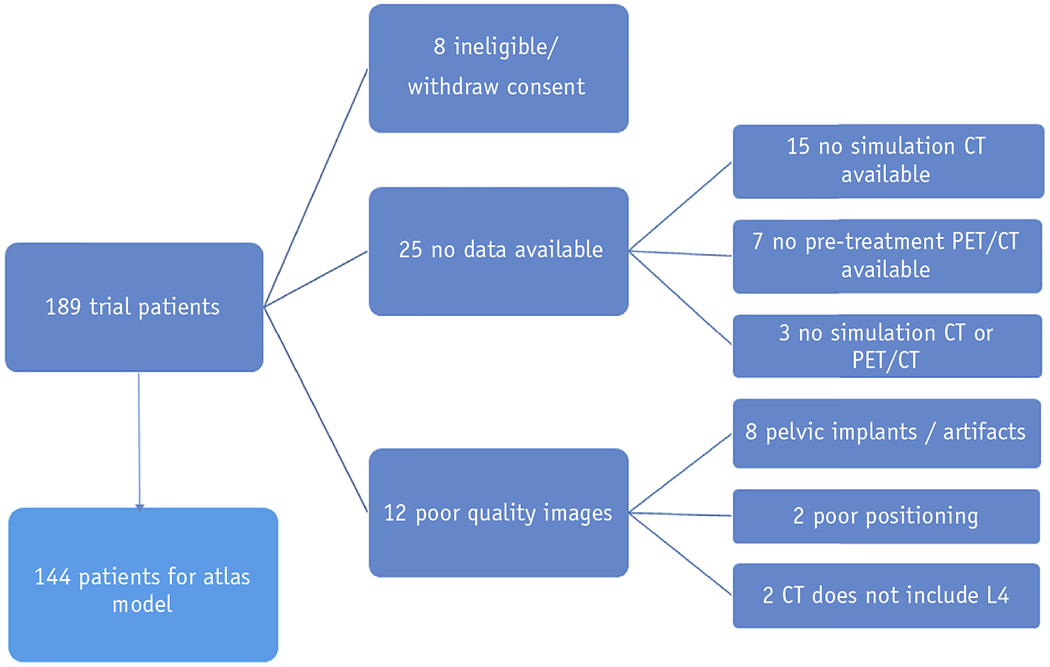
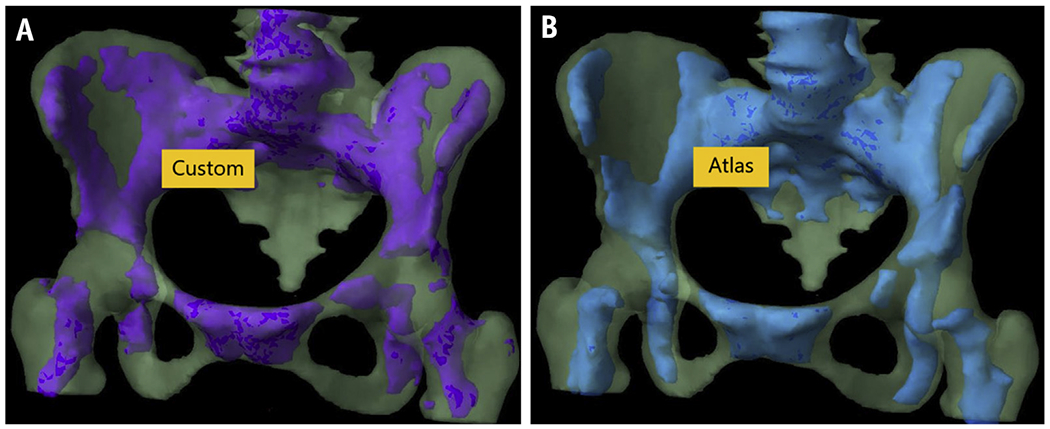
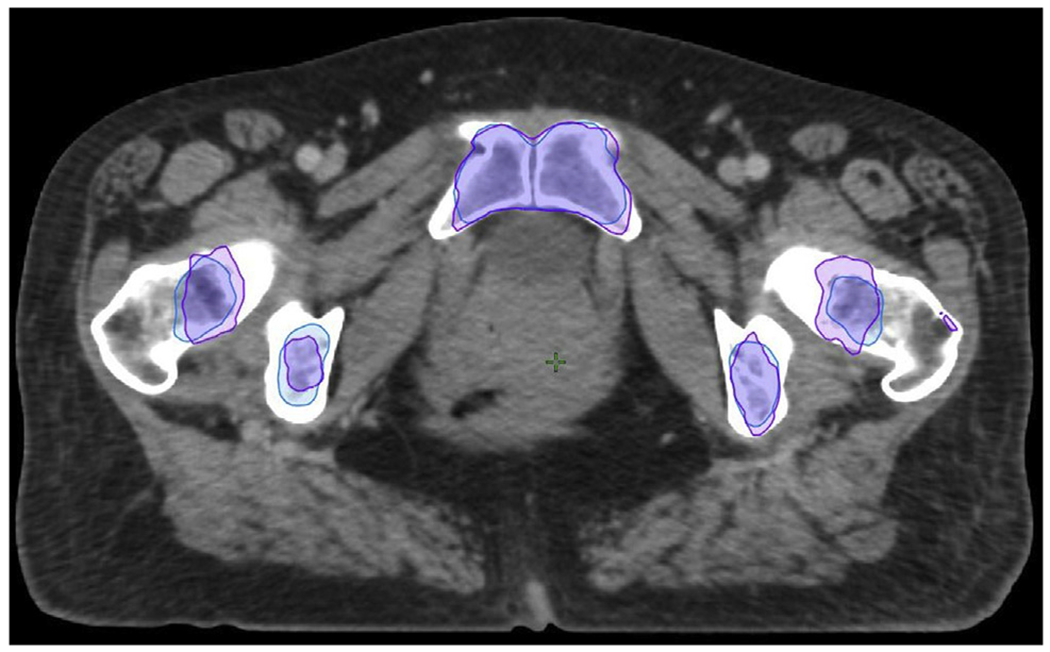
Methods and materials: A multiatlas was built on a training set of 144 patients and validated in 32 patients from the NRG-GY006 clinical trial. ABM for individual patients was defined as the subvolume of pelvic bone greater than the individual mean standardized uptake value on registered 18F-fluorodeoxyglucose PET/CT images. Atlas-based and custom ABM segmentations were compared using the Dice similarity coefficient and mean distance to agreement and used to generate ABM-sparing intensity modulated radiation therapy plans. Dose-volume metrics and normal tissue complication probabilities of the two approaches were compared using linear regression.
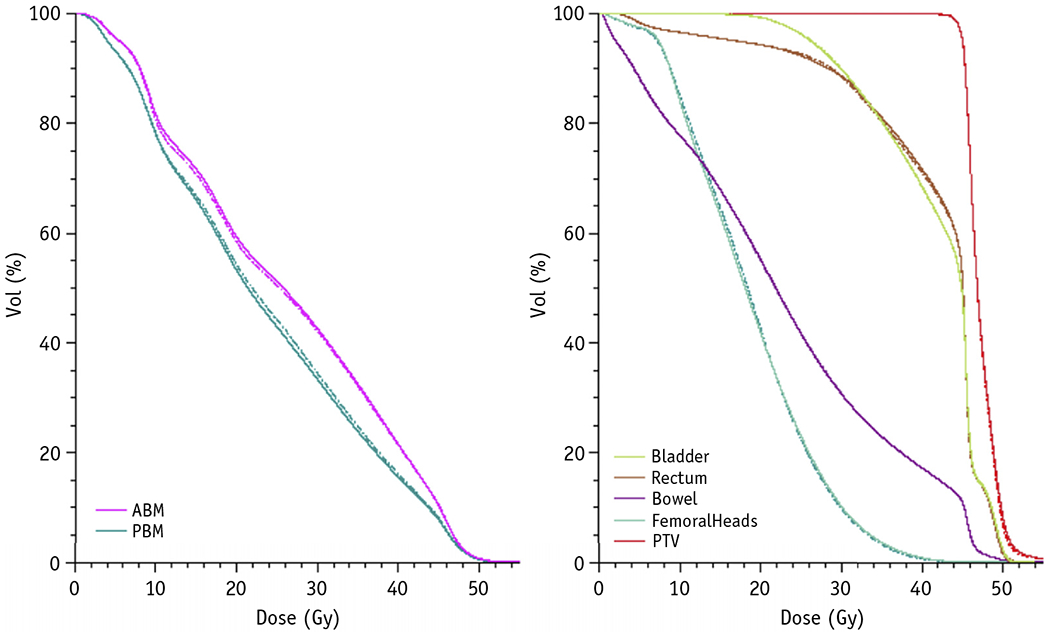
Results: Atlas-based ABM volumes (mean [standard deviation], 548.4 [88.3] cm3) were slightly larger than custom ABM volumes (535.1 [93.2] cm3), with a Dice similarity coefficient of 0.73. Total pelvic bone marrow V20 and Dmean were systematically higher and custom ABM V10 was systematically lower with custom-based plans (slope: 1.021 [95% confidence interval (CI), 1.005-1.037], 1.014 [95% CI, 1.006-1.022], and 0.98 [95% CI, 0.97-0.99], respectively). We found no significant differences between atlas-based and custom-based plans in bowel, rectum, bladder, femoral heads, or target dose-volume metrics.
Conclusions: Atlas-based ABM segmentation can reduce pelvic bone marrow dose while achieving comparable target and other normal tissue dosimetry. This approach may allow ABM sparing in settings where PET/CT is unavailable.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
-
- Torres MA, Jhingran A, Thames HD, et al. Comparison of treatment tolerance and outcomes in patients with cervical cancer treated with concurrent chemoradiotherapy in a prospective randomized trial or with standard treatment. Int J Radiat Oncol Biol Phys 2008;70:118–125. - PubMed
-
- Mell LK, Kochanski JD, Roeske JC, et al. Dosimetric predictors of acute hematologic toxicity in cervical cancer patients treated with concurrent cisplatin and intensity-modulated pelvic radiotherapy. Int J Radiat Oncol Biol Phys 2006;66:1356–1365. - PubMed
-
- Yang Y, Li W, Qian J, Zhang J, Shen Y, Tian Y. Dosimetric predictors of acute hematologic toxicity due to intensity-modulated pelvic radiotherapy with concurrent chemotherapy for pelvic cancer patients. Transl Cancer Res 2018;7:515–523.
-
- Albuquerque K, Giangreco D, Morrison C, et al. Radiation-related predictors of hematologic toxicity after concurrent chemoradiation for cervical cancer and implications for bone marrow–sparing pelvic IMRT Int J Radiat Oncol 2011;79:1043–1047. - PubMed
