

Behçet's Uveitis: Current Diagnostic and Therapeutic Approach
- PMID: 32631005
- PMCID: PMC7338748
- DOI: 10.4274/tjo.galenos.2019.60308
Behçet's Uveitis: Current Diagnostic and Therapeutic Approach
Abstract
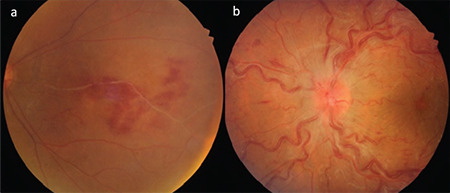
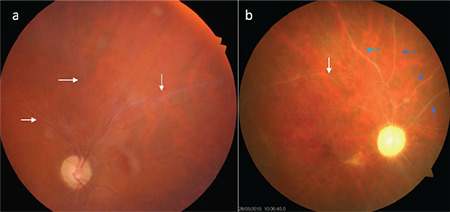
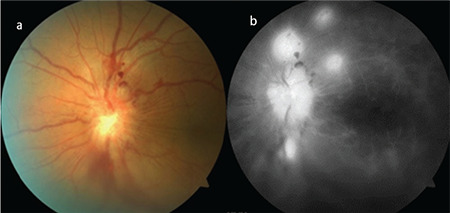
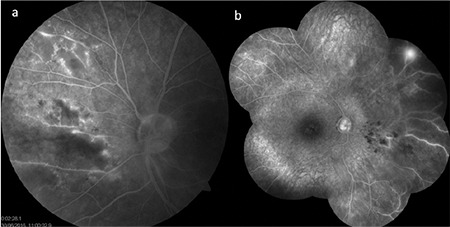
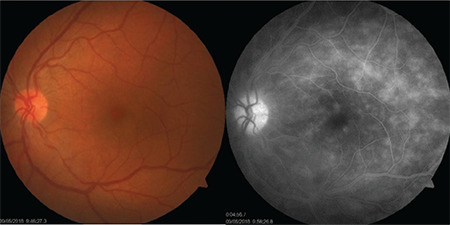
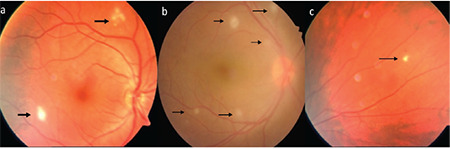
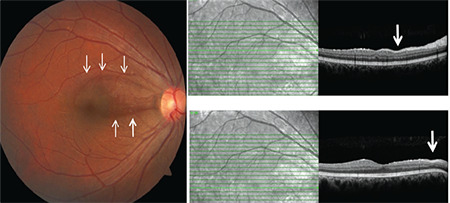
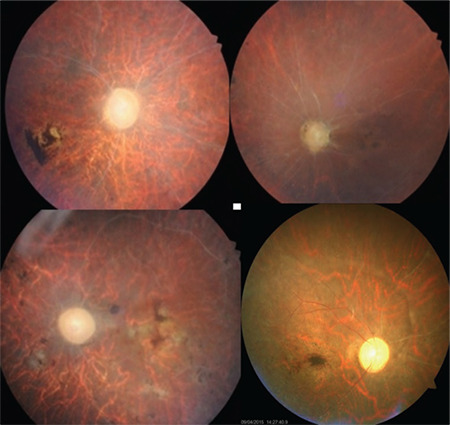
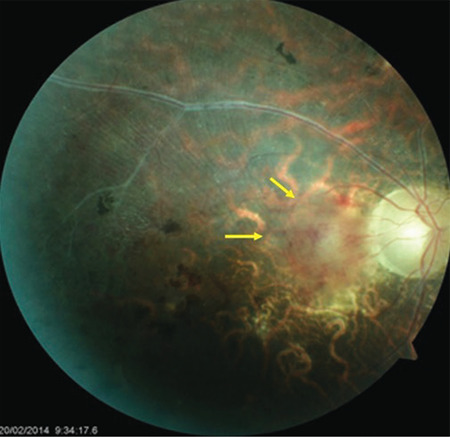
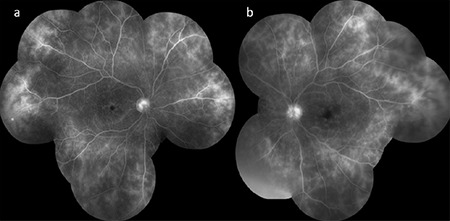
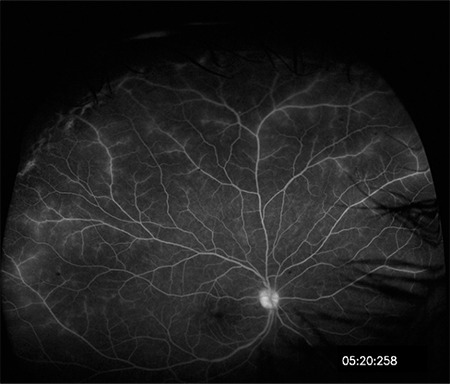
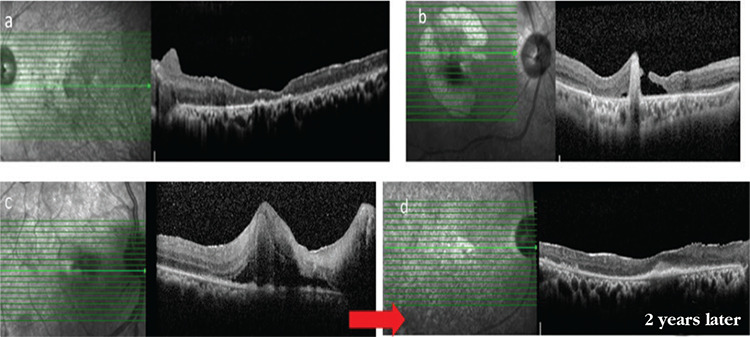
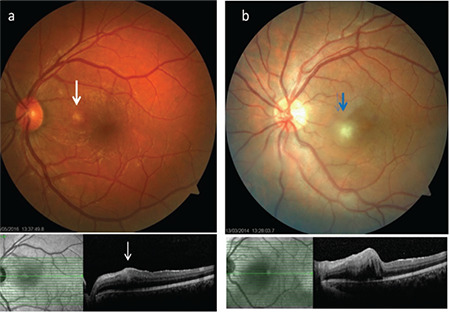
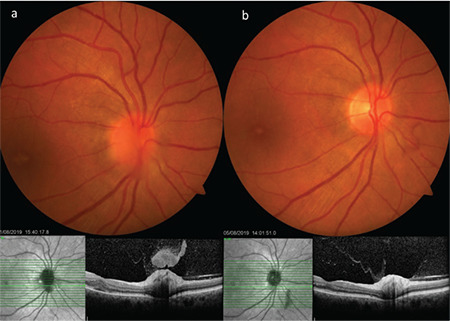
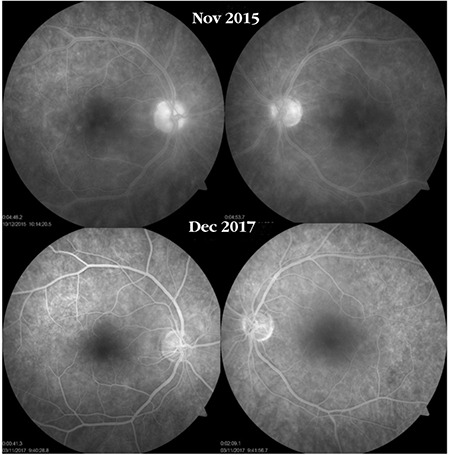
Behçet's disease is a chronic, multisystem inflammatory disorder characterized by relapsing inflammation. Although its etiopathogenesis has not yet been clarified, both the adaptive and innate immune systems, genetic predisposition, and environmental factors have all been implicated. It is more frequent and more severe in males in the third and fourth decades of life. The eye is the most frequently involved organ in the course of the disease. Ocular involvement (Behçet's uveitis) is characterized by bilateral recurrent non-granulomatous panuveitis and occlusive retinal vasculitis. Recurrent inflammatory episodes in the posterior segment may lead to permanent vision loss due to irreversible retinal damage and complications such as macular scarring, macular atrophy, and optic atrophy. Early and aggressive immunomodulatory treatment and the use of biologic agents when needed are crucial for preventing recurrences and improving visual prognosis.
Keywords: Behçet’s uveitis; biologics; imaging; prognosis; treatment.
Figures
References
-
- Behçet H. Über rezidivierende aphthöse durch ein Virus verursachte Geschwüre am Mund, am Auge und an den Genitalien. Dermatol Wochenschr. 1937;105:1152–1157.
-
- Khairallah M, Accorinti M, Muccioli C, Kahloun R, Kempen JH. Epidemiology of Behçet disease. Ocul Immunol Inflamm. 2012;20:324–335. - PubMed
-
- Azizlerli G, Köse AA, Sarica R, Gül A, Tutkun IT, Kulaç M, Tunç R, Urgancioğlu M, Dişçi R. Prevalence of Behçet’s disease in Istanbul, Turkey. Int J Dermatol. 2003;42:803–806. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical