

Chronic pain after groin hernia repair: pain characteristics and impact on quality of life
- PMID: 32631293
- PMCID: PMC7336434
- DOI: 10.1186/s12893-020-00805-9
Chronic pain after groin hernia repair: pain characteristics and impact on quality of life
Abstract
Background: Chronic postsurgical pain (CPSP) after hernia repair research has mainly relied on unconfirmed self-reporting. We aimed to describe confirmed CPSP incidence, management, and quality of life (QoL) in a 2-year prospective study.
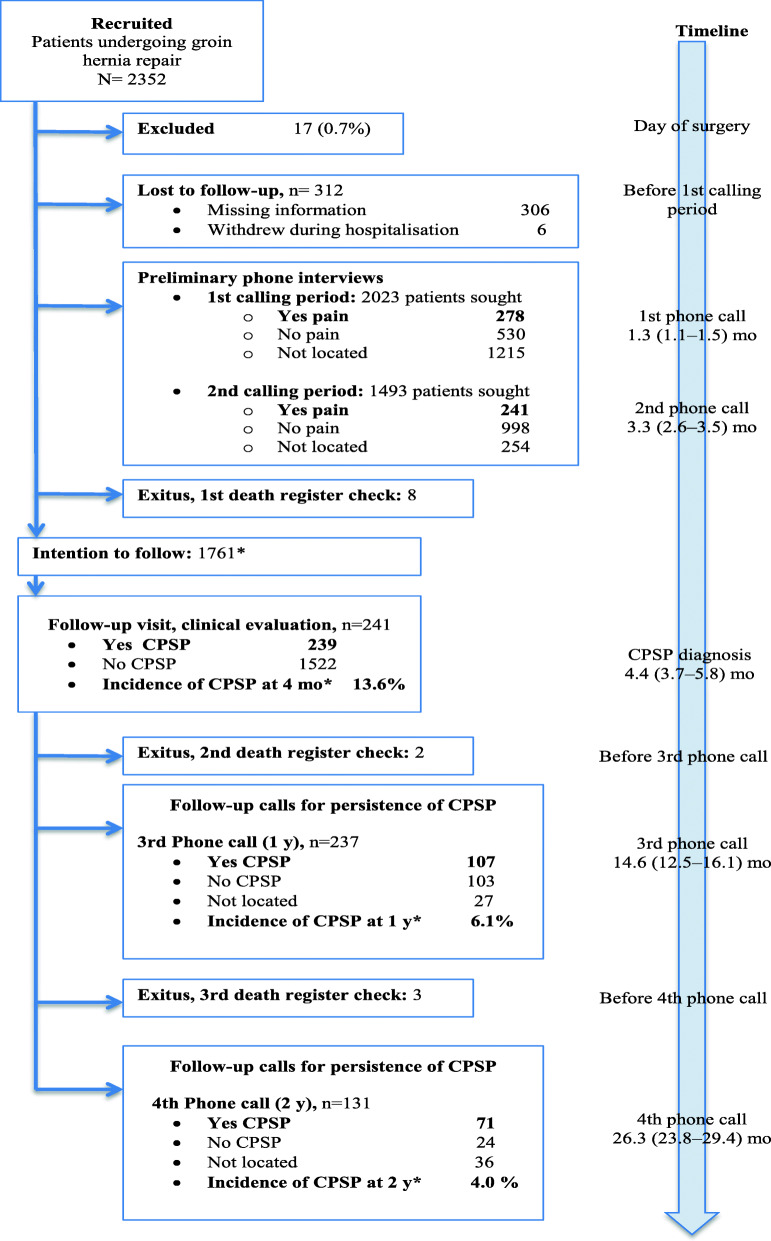
Methods: Multicenter study (GENDOLCAT) of 3890 patients undergoing 4 common surgical procedures in 23 hospitals to develop a risk model for CPSP; 2352 men underwent open hernia repair. Patients with pain were identified by telephone at 1 and 3 months and referred to the hospital 4 months after surgery for a physical examination to confirm CPSP. Three validated tools were used: the Brief Pain Inventory (BPI) for severity, analgesic use, and interference with activities; the SF-12 questionnaire for QoL (validated Spanish version), and the Douleur Neuropathique 4 (DN4). Patients with CPSP were called again at 1 and 2 years.
Results: In 1761 patients who underwent hernia repair and were eligible for physical examination for CPSP, the incidence of confirmed pain at 4 months was 13.6% (patient-reported pain, 6.2% at 1 year and 4.0% at 2 years). Neuropathic pain was diagnosed in 38.5% of the CPSP patients at 4 months. The incidences of neuropathic CPSP in patients with mesh or non-mesh repairs were similar (38.6 and 33.3%, respectively). SF-12 physical component scores changed little in all patients, whether or not they developed CPSP. The SF-12 mental component decreased significantly in all patients, but the decrease was clinically significant only in CPSP patients. CPSP interfered with activities (18%), work (15.6%), walking (15%) and mood (10.2%). At 2 years 52.1% of CPSP patients had moderate/intense pain and 28.2% took analgesics.
Conclusion: CPSP affects QoL-related activities, and although it diminishes over the course of 2 years after surgery, many patients continue to have moderate/intense pain and take analgesics. CPSP and neuropathic pain rates seem to be similar after mesh and non-mesh repair. BPI and SF-12 mental component scores detect effects on QoL.
Trial registration: ClinicalTrials.gov NCT01510496.
Keywords: Chronic pain; Hernia repair; Quality o life.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Montes A, Roca G, Sabate S, Lao JI, Navarro A, Cantillo J, Canet J, GENDOLCAT Study Group Genetic and clinical factors associated with chronic postsurgical pain after hernia repair, hysterectomy, and thoracotomy: a two-year multicenter cohort study. Anesthesiology. 2015;122:1123–1141. doi: 10.1097/ALN.0000000000000611. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
