

Mapping male circumcision for HIV prevention efforts in sub-Saharan Africa
- PMID: 32631314
- PMCID: PMC7339571
- DOI: 10.1186/s12916-020-01635-5
Mapping male circumcision for HIV prevention efforts in sub-Saharan Africa
Abstract
Background: HIV remains the largest cause of disease burden among men and women of reproductive age in sub-Saharan Africa. Voluntary medical male circumcision (VMMC) reduces the risk of female-to-male transmission of HIV by 50-60%. The World Health Organization (WHO) and Joint United Nations Programme on HIV/AIDS (UNAIDS) identified 14 priority countries for VMMC campaigns and set a coverage goal of 80% for men ages 15-49. From 2008 to 2017, over 18 million VMMCs were reported in priority countries. Nonetheless, relatively little is known about local variation in male circumcision (MC) prevalence.
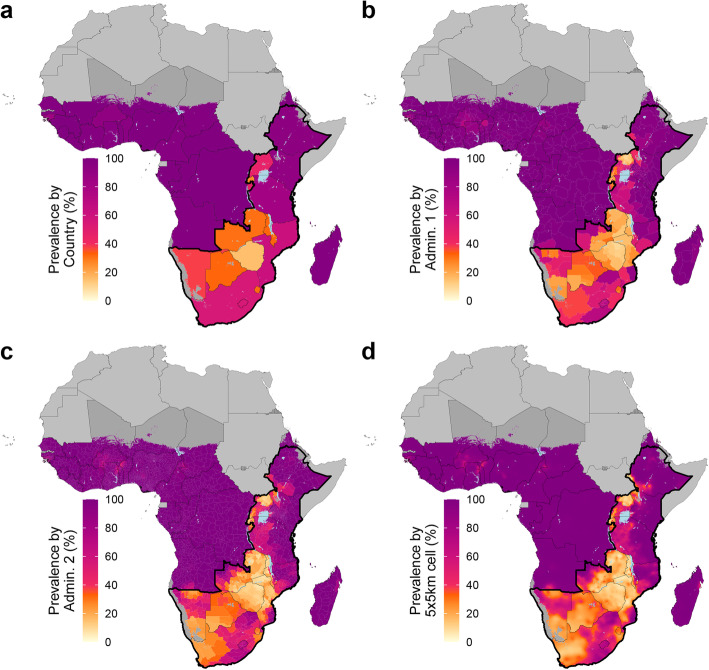
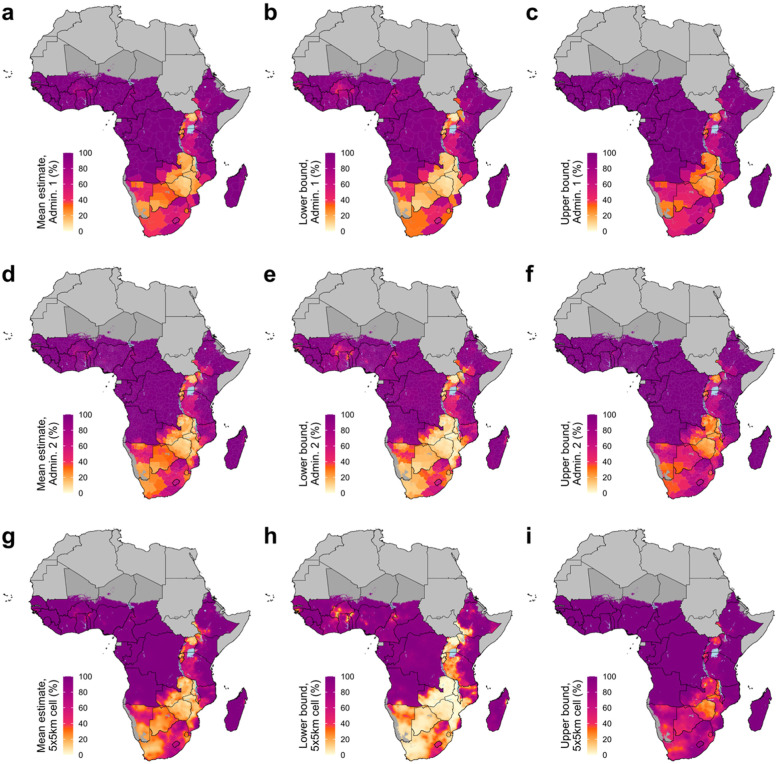
Methods: We analyzed geo-located MC prevalence data from 109 household surveys using a Bayesian geostatistical modeling framework to estimate adult MC prevalence and the number of circumcised and uncircumcised men aged 15-49 in 38 countries in sub-Saharan Africa at a 5 × 5-km resolution and among first administrative level (typically provinces or states) and second administrative level (typically districts or counties) units.
Results: We found striking within-country and between-country variation in MC prevalence; most (12 of 14) priority countries had more than a twofold difference between their first administrative level units with the highest and lowest estimated prevalence in 2017. Although estimated national MC prevalence increased in all priority countries with the onset of VMMC campaigns, seven priority countries contained both subnational areas where estimated MC prevalence increased and areas where estimated MC prevalence decreased after the initiation of VMMC campaigns. In 2017, only three priority countries (Ethiopia, Kenya, and Tanzania) were likely to have reached the MC coverage target of 80% at the national level, and no priority country was likely to have reached this goal in all subnational areas.
Conclusions: Despite MC prevalence increases in all priority countries since the onset of VMMC campaigns in 2008, MC prevalence remains below the 80% coverage target in most subnational areas and is highly variable. These mapped results provide an actionable tool for understanding local needs and informing VMMC interventions for maximum impact in the continued effort towards ending the HIV epidemic in sub-Saharan Africa.
Keywords: Africa; Geospatial; Geostatistics; HIV; HIV prevention; Intervention; Male circumcision; Mapping; Medical male circumcision; Spatial statistics; Voluntary medical male circumcision.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- James SL, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- World Health Organization. Voluntary medical male circumcision for HIV prevention. 2018. https://www.who.int/hiv/pub/malecircumcision/vmmc-progress-brief-2018/en/. Accessed 29 Apr 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
