

Add-on therapy in metformin-treated patients with type 2 diabetes at moderate cardiovascular risk: a nationwide study
- PMID: 32631337
- PMCID: PMC7339487
- DOI: 10.1186/s12933-020-01078-5
Add-on therapy in metformin-treated patients with type 2 diabetes at moderate cardiovascular risk: a nationwide study
Abstract
Background: In randomised clinical trials, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium-glucose cotransporter 2 (SGLT-2) inhibitors reduced cardiovascular events in patients with type 2 diabetes (T2D) at high cardiovascular risk, as compared to standard care. However, data comparing these agents in patients with T2D who are at moderate risk is sparse.
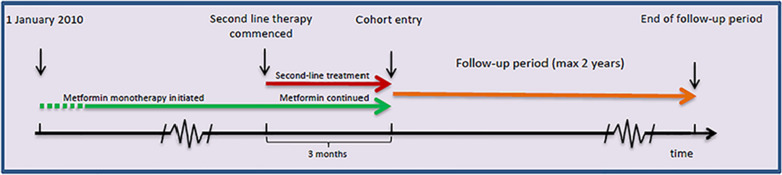
Methods: From Danish national registries, we included patients with T2D previously on metformin monotherapy, who started an additional glucose-lowering agent [GLP-1 RA, SGLT-2 inhibitor, dipeptidyl peptidase-4 (DPP-4) inhibitor, sulfonylurea (SU), or insulin] in the period 2010-2016. Patients with a history of cardiovascular events [heart failure (HF), myocardial infarction (MI) or stroke] were excluded. Patients were followed for up to 2 years. Cause-specific adjusted Cox regression models were used to compare the risk of hospitalisation for HF, a composite endpoint of major adverse cardiovascular events (MACE) (MI, stroke or cardiovascular death), and all-cause mortality for each add-on therapy. Patients who initiated DPP-4 inhibitors were used as reference.
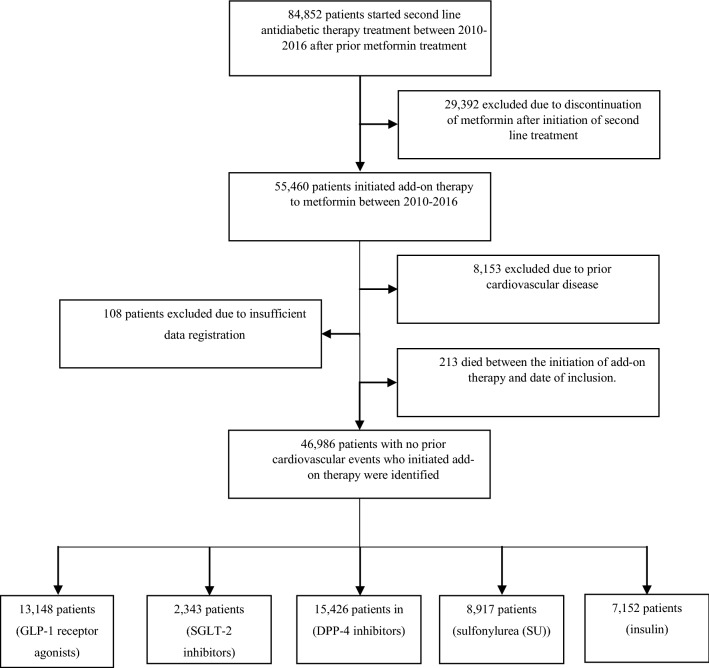
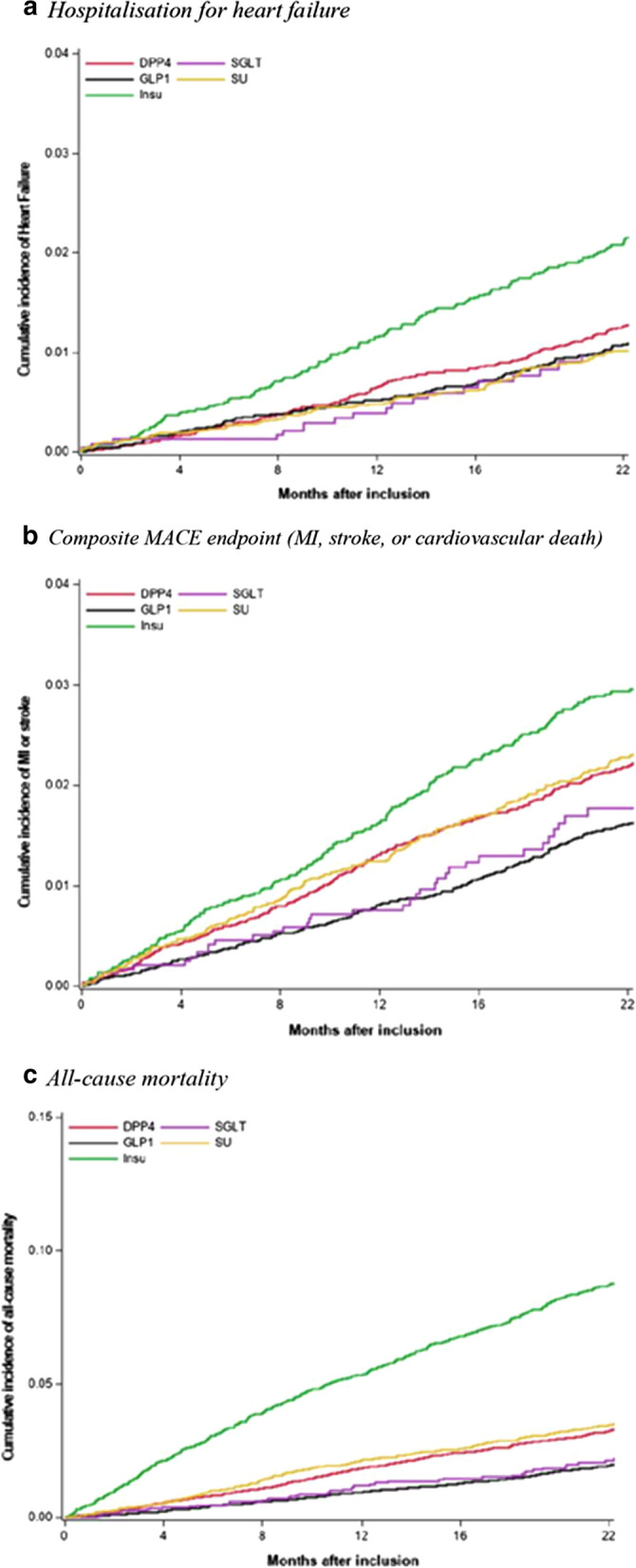
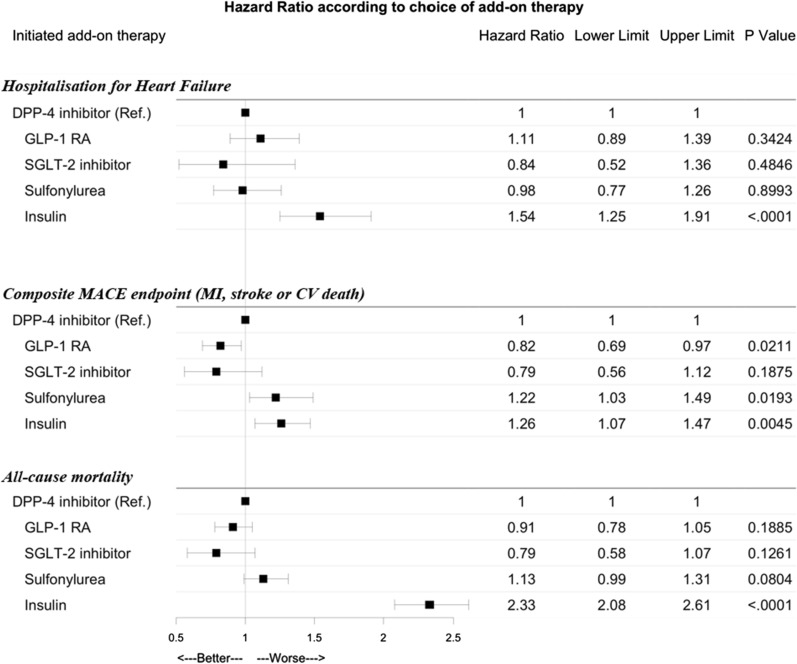
Results: The study included 46,986 T2D patients with a median age of 61 years and of which 59% were male. The median duration of metformin monotherapy prior to study inclusion was 5.3 years. Add-on therapy was distributed as follows: 13,148 (28%) GLP-1 RAs, 2343 (5%) SGLT-2 inhibitors, 15,426 (33%) DPP-4 inhibitors, 8917 (19%) SUs, and 7152 (15%) insulin. During follow-up, 623 (1.3%, range 0.8-2.1%) patients were hospitalised for HF-hazard ratios (HR) were 1.11 (95% CI 0.89-1.39) for GLP-1 RA, 0.84 (0.52-1.36) for SGLT-2 inhibitors, 0.98 (0.77-1.26) for SU and 1.54 (1.25-1.91) for insulin. The composite MACE endpoint occurred in 1196 (2.5%, range 1.5-3.6%) patients, yielding HRs of 0.82 (0.69-0.97) for GLP-1 RAs, 0.79 (0.56-1.12) for SGLT-2 inhibitors, 1.22 (1.03-1.49) for SU and 1.23 (1.07-1.47) for insulin. 1865 (3.9%, range 1.9-9.0%) died from any cause during follow-up. HRs for all-cause mortality were 0.91 (0.78-1.05) for GLP-1 RAs, 0.79 (0.58-1.07) for SGLT-2 inhibitors, 1.13 (0.99-1.31) for SU and 2.33 (2.08-2.61) for insulin.
Conclusion: In a nationwide cohort of metformin-treated T2D patients and no history of cardiovascular events, the addition of either GLP-1 RA or SGLT-2 inhibitor to metformin treatment was associated with a similar risk of hospitalisation for HF and death, and a lower risk of MACE for GLP-1 RA when compared with add-on DPP-4 inhibitors. By contrast, initiation of treatment with SU and insulin were associated with a higher risk of MACE. Additionally, insulin was associated with an increased risk of all-cause mortality and hospitalisation for HF.
Keywords: Heart failure; Myocardial infarction; Prognosis; Treatment; Type 2 diabetes.
Conflict of interest statement
Dr. Køber reports receiving lecture fees from Sanofi and Novartis; Dr. Torp-Pedersen, lecture fees and grant support from Bayer. No other potential conflict of interest relevant to this article was reported.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
