

The feasibility of non-contrast enhanced plus contrast-enhanced computed tomography in discriminating invasive pure ground-glass opacity from pre-invasive pure ground-glass opacity
- PMID: 32631446
- PMCID: PMC7336435
- DOI: 10.1186/s13019-020-01159-2
The feasibility of non-contrast enhanced plus contrast-enhanced computed tomography in discriminating invasive pure ground-glass opacity from pre-invasive pure ground-glass opacity
Abstract
Background: Invasive pure ground-glass opacity and pre-invasive pure ground-glass opacity have different 5-year overall survival rate and risk of lymph node metastasis and the extent of resection. It is difficult to discriminate these nodules since they share similar CT features and may occur concurrently. The objectives of this study were to investigate the feasibility of non-contrast enhanced plus contrast-enhanced computed tomography in discriminating invasive pure ground-glass opacity from pre-invasive pure ground-glass opacity.
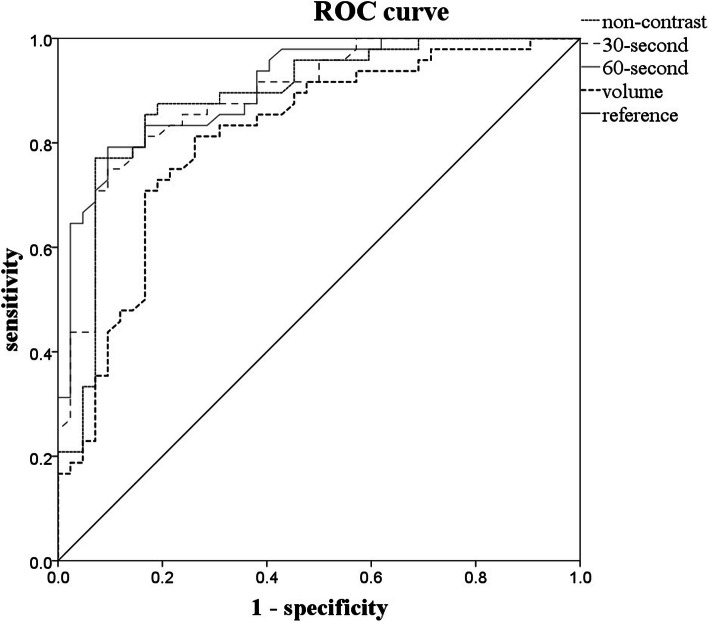
Methods: We retrospectively examined 90 patients with pure ground-glass opacity who underwent non-contrast enhanced and contrast-enhanced CT according to a simplified protocol (one non-contrast enhanced measurement and two contrast-enhanced measurements at 30 s and 60 s after contrast injection) from 2015 to 2019. All imaging examinations were analyzed using three-dimensional computer-aided volume. Two independent samples t tests, one-way analysis of variance, chi-square test and logistic regression were used for analysis. A receiver operating characteristic curve was used to determine the optimal cut-off value of mean CT attenuation for differentiation of groups and to obtain diagnostic value.
Results: (1) The CT values of one non-contrast-enhanced, two contrast-enhanced and volume measurements between two groups had statistically significant differences (P < 0.001). (2) At the 30-s scan, there were more nodules in the pre-invasive group with no enhancement than in the pre-invasive group, which was statistically significant. (3) The CT value of 60-s scan was independent predictor of invasive adenocarcinoma (P = 0.019).
Conclusions: Non-contrast enhanced plus two contrast-enhanced CT based on volume measurements can differentiate invasive pGGO from pre-invasive pGGO.
Keywords: Adenocarcinoma; Ground-grass opacity (GGO); Mean computer tomography value; Volumetric CT.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6:244–285. doi: 10.1097/JTO.0b013e318206a221. - DOI - PMC - PubMed
-
- Ye XD, Yuan Z, Ye JD, Li HM, Xiao XS. Dynamic enhanced CT evaluation of solitary pulmonary nodules. Zhonghua Zhong Liu Za Zhi. 2011;33:308–312. - PubMed
-
- Cheng X, Zheng D, Li Y, Li H, Sun Y, Xiang J, Chen H. Tumor histology predicts mediastinal nodal status and may be used to guide limited lymphadenectomy in patients with clinical stage I non-small cell lung cancer. J Thorac Cardiovasc Surg. 2018;155:2648–2656. doi: 10.1016/j.jtcvs.2018.02.010. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
