

Editorial
doi: 10.1016/j.jtcvs.2020.05.083.
Epub 2020 Jun 6.
Molecular chronicles of cytokine burst in patients with coronavirus disease 2019 (COVID-19) with cardiovascular diseases
Affiliations
- PMID: 32631657
- PMCID: PMC7834736
- DOI: 10.1016/j.jtcvs.2020.05.083
Item in Clipboard
Editorial
Molecular chronicles of cytokine burst in patients with coronavirus disease 2019 (COVID-19) with cardiovascular diseases
J Thorac Cardiovasc Surg.
2021 Feb.
No abstract available
Figures
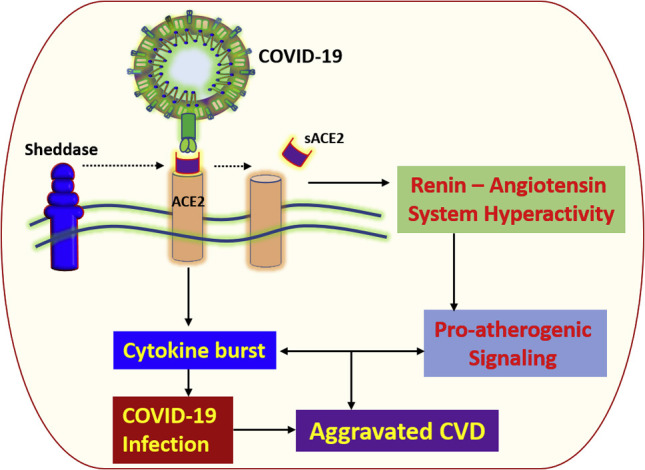
Biochemical events and molecular transit in aggravated COVID-19–CVD comorbidity.
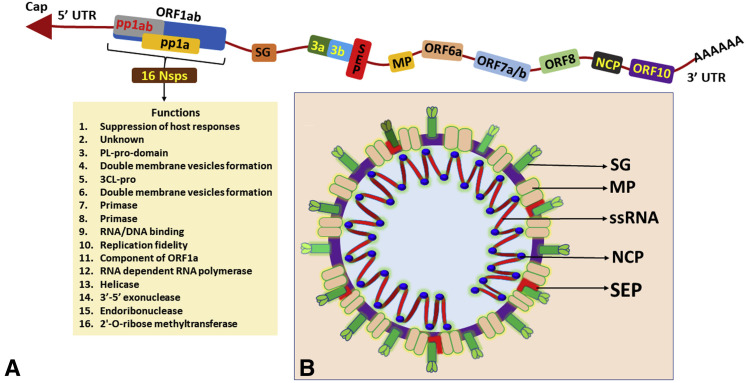
A, Genomic organization of COVID-19. The COVID-19 genome contains 6-11 ORFs where the two-thirds of viral genome is contained in the first ORF (ORF1a/b), which codes for 2 polyproteins (pp1a and pp1ab) and 16 Nsps. The genome of COVID-19 is organized in the order of 5′-orf1/ab (replicase)-structural proteins (SG-SEP-MP-NCP)-3′. B, Structural organization of COVID-19: COVID-19 exists in round, elliptic, and pleomorphic morphology with average diameter of 60 to 140 nm. The structural and accessory proteins including SG, SEP, NCP, and MP. ORF, Open reading frame; Nsp, non-structural protein; SG, spike glycoprotein; SEP, small envelope protein; MP, matrix protein; NCP, nucleocapsid protein.
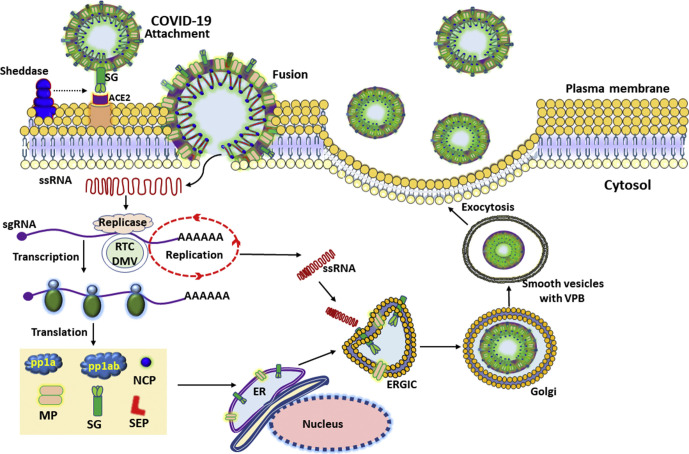
Pathology of COVID-19 infection. SG mediates the attachment of COVID-19 to its receptor, ACE2, in the plasma membrane of alveolar cells. The binding is facilitated by the sheddases (ADAM metallopeptidase domain-17/CTSL/transmembrane protease/serine subfamily member 2), leading to the membrane fusion between COVID-19 and host cells. The S1 subunit of SG is involved in the high-affinity binding of COVID-19 to the ACE2 receptor, whereas the S2 subunit facilitates the membrane fusion by harboring essential mediators. Following membrane fusion, the viral genome is released to the cytosol, where uncoated viral genome initiates the translation of pp1a and pp1ab. The pp1a and pp1ab code for non-structural proteins required for the assembly of RTC in DMV. Immediately following the assembly, the RTC initiates the replication of viral RNA to synthesize a battery of sgRNAs encoding the structural and accessory proteins. Finally, employing the host ER and Golgi machinery, the newly formed viral genome and proteins assemble to form VPBs. VPBs are virion containing vesicles that ultimately fuse with the host cell plasma membrane to release virus. COVID-19, Coronavirus disease 2019; SG, spike glycoprotein; ACE2, angiotensin-converting enzyme 2; sgRNA, subgenomic RNA; RTC, replication transcription complex; DMV, double-membrane vesicle; ER, endoplasmic reticulum; VPB, viral particle buds; MP, matrix protein; SG, spike glycoprotein; NCP, nucleocapsid protein; SEP, small envelope protein; ERGIC, ER-Golgi intermediate compartment.
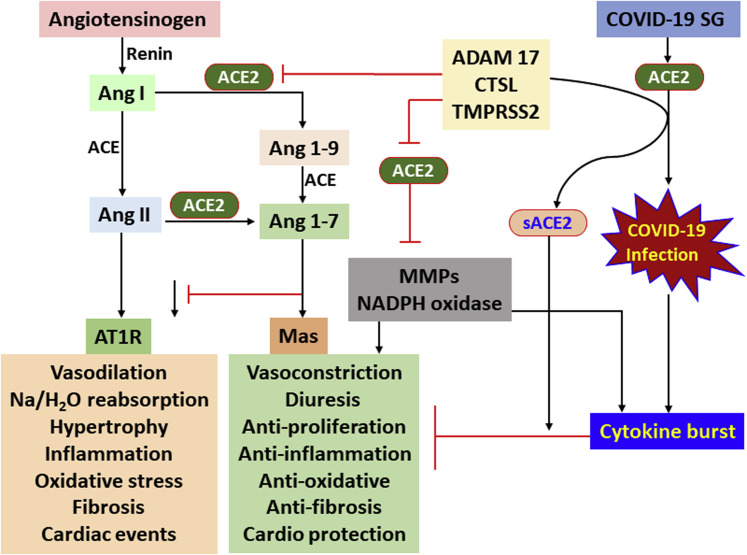
ACE2 signaling in CVD versus COVID-19 infection. ACE2 proteolytically inactivates Ang I and Ang II and acts on Ang I to form Ang 1-9 peptide, which is the precursor of the vasodilator Ang 1-7. The binding of Ang II with type-1 receptors (AT1R and AT2R) initiates a series of biochemical events leading to vasoconstriction, oxidative stress, fibrosis, and retention of electrolytes. In contrast, ACE2–Ang 1-7 axis via G-protein coupled protein receptor (Mas) acts as counter-regulator by promoting vasodilation, antioxidant responses, and antifibrotic reactions. The decline of ACE2 expression following the progression of CVDs enhances the myocardial dysfunction and induces inflammatory burden. The decreased ACE2 activity results in the activation of myocardial NADPH oxidase system, leading to superoxide-activated oxidative stress and hyperactivation of MMPs, which subsequently aggravate CVD pathology. The COVID-19 SG increases the susceptibility of SG to undergo proteolytic cleavage by sheddases, including ADAM-17, CTSL, and TMPRSS2, which is essential for coronavirus entry to the host cells. The shedding of ACE2 results in the suppression of downstream signaling, leading to increased Ang II level and subsequent aggravation of CVD pathology. sACE2 is associated with aggravated CVD pathology. Ang, Angiotensin; ACE2, angiotensin-converting enzyme 2; COVID-19, coronavirus disease 2019; SG, spike glycoprotein; ADAM-17, ADAM metallopeptidase domain-17; CTSL, cysteine protease cathepsin L; TMPRSS2, transmembrane protease/serine subfamily member 2; MMP, matrix metallopeptidase; NADPH, nicotinamide adenine dinucleotide phosphate.
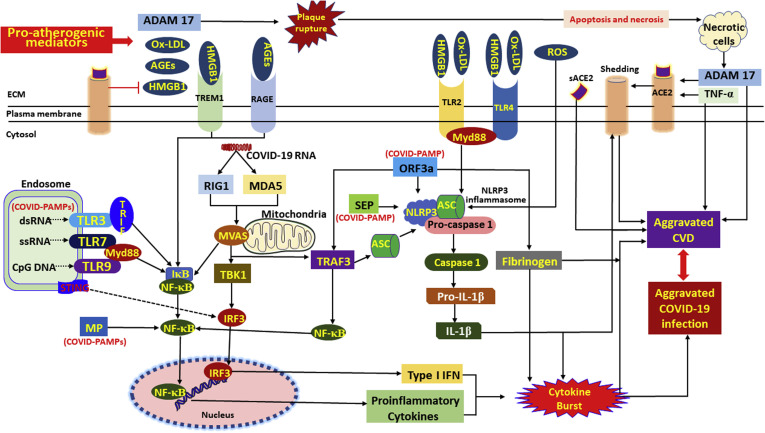
Proposed molecular mechanism underlying aggravated inflammatory response in COVID-19–CVD comorbidity. The components of COVID-19, including the RNA and proteins, act as intracellular PAMPs, which are recognized by conventional pattern recognition receptors, especially TLRs, RIG-I-like receptors (RLRs), and NLRP3 inflammasome. The TLRs, including TLR3, TLR7, TLR8, and TLR9, detect viral genome in the endosomal vesicles. In addition, the viral genome in the cytosol are recognized by the cytosolic receptors including RIG-1 and MDA5. The binding of viral ligands with the receptors initiates the recruitment and assembly of adaptor proteins including TRIF, MAVS, and STING, which trigger the activation of the transcription factor NF-κB and IRF3 via MyD88 adapter. IRF3 triggers the expression of type I IFNs, whereas NF-κB stimulates the expression of a battery of proinflammatory cytokines leading to cytokine burst. IL-1β is generated by the proteolytic activation of pro–IL-1β by caspase-1 following the activation of NLRP3 inflammasome. The active NLRP3 inflammasome upregulates the transcription of pro–IL-1β gene and subsequent activation by caspase-1. The COVID-19 proteins including MP, SEP, and ORF3a activate NLRP3 via TRAF3 and subsequent IL-1β and ORF3a activate NF-κB and downstream cytokine burst. The apoptotic/necrotic cells following virus infection upregulate ADAM-17, the major sheddase for ACE2. IL-1β and TNF-α enhance the ACE2 shedding. The resultant sACE2 is a potent mediator for vascular inflammation and CVD pathology. ADAM-17 activates atherosclerotic plaque rupture and vascular inflammation. ACE2 inhibits the DAMPs, including HMGB1 released from the infected and ischemic/necrotic cells due to membrane damage. The decreased levels of ACE2 lead to increased DAMPs, especially OxLDL, HMGB1, AGEs, and ROS. These mediators trigger NLRP3 inflammasome via TLR2, TLR4, RAGE, and/or TREM1 axes in cardiovascular system. The upregulation of such DAMPs in the ACE2-depleted environment is detrimental, resulting in aggravated COVID-19–CVD comorbidity. ADAM-17, ADAM metallopeptidase domain-17; OxLDL, oxidized low-density lipoprotein; AGEs, advanced glycation end products; HMGB1, high mobility group box 1; TLR, Toll-like receptor; ROS, reactive oxygen species; ACE2, angiotensin-converting enzyme 2; TNF-α, tumor necrosis factor-α; COVID-19, coronavirus disease 2019; TRIF, TIR-domain-containing adaptor protein including IFN-β; RIG-1, retinoic acid-inducible gene 1; MDA5, melanoma differentiation-associated gene 5; STING, stimulator of interferon genes protein; MP, matrix protein; MAV, mitochondrial antiviral-signaling protein; TRAF3, TNF receptor-associated factor; PAMPs, pathogen-associated molecular patterns; NF-κB, nuclear factor-κB; IRF3, interferon regulatory factor 3; ORF, open reading frame; SEP, small envelope protein; NLRP3, Nod-like receptor protein 3; IL, interleukin; IFN, interferon; CVD, cardiovascular disease.
Comment in
-
Commentary: The molecular pandemonium of coronavirus disease 2019.J Thorac Cardiovasc Surg. 2021 Feb;161(2):e227-e228. doi: 10.1016/j.jtcvs.2020.06.003. Epub 2020 Jun 6. J Thorac Cardiovasc Surg. 2021. PMID: 32624308 Free PMC article. No abstract available.
-
Commentary: Evolving understanding of coronavirus disease 2019: Molecular biology, immunology, and surgery.J Thorac Cardiovasc Surg. 2021 Feb;161(2):e228-e230. doi: 10.1016/j.jtcvs.2020.05.087. Epub 2020 Jun 6. J Thorac Cardiovasc Surg. 2021. PMID: 32631659 Free PMC article. No abstract available.
References
-
- COVID-19 Coronavirus (COVID-19) map. https://google.com/covid19-map Available at:
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
