

Recommendations for the management of cardiovascular risk in patients with chronic myeloid leukemia on tyrosine kinase inhibitors: risk assessment, stratification, treatment and monitoring
- PMID: 32631809
- PMCID: PMC8211634
- DOI: 10.1016/j.htct.2020.04.009
Recommendations for the management of cardiovascular risk in patients with chronic myeloid leukemia on tyrosine kinase inhibitors: risk assessment, stratification, treatment and monitoring
Abstract
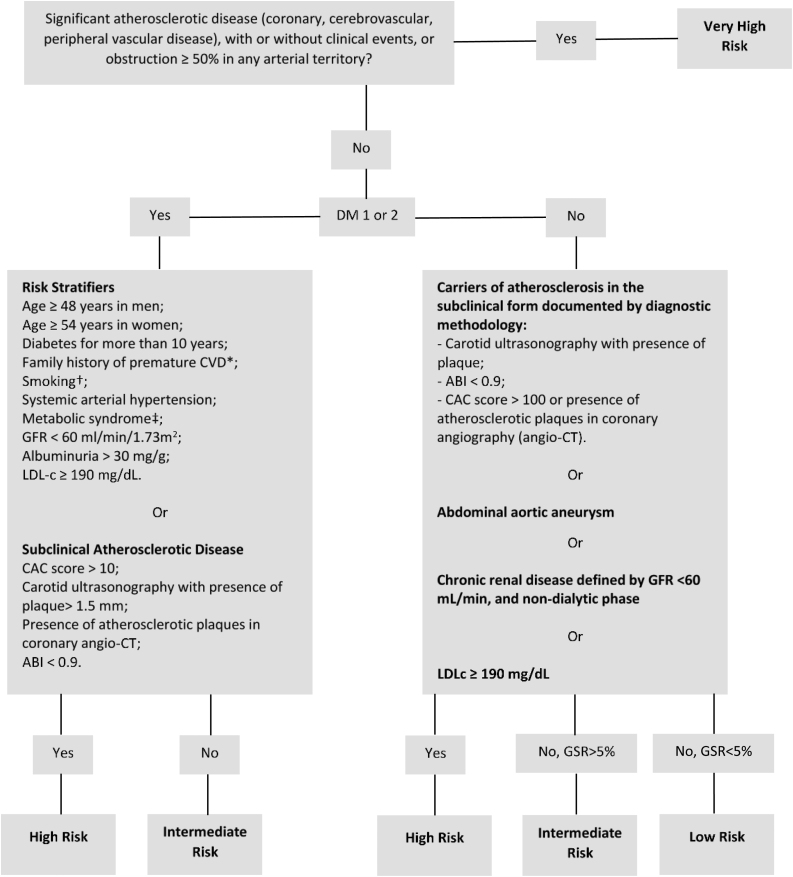
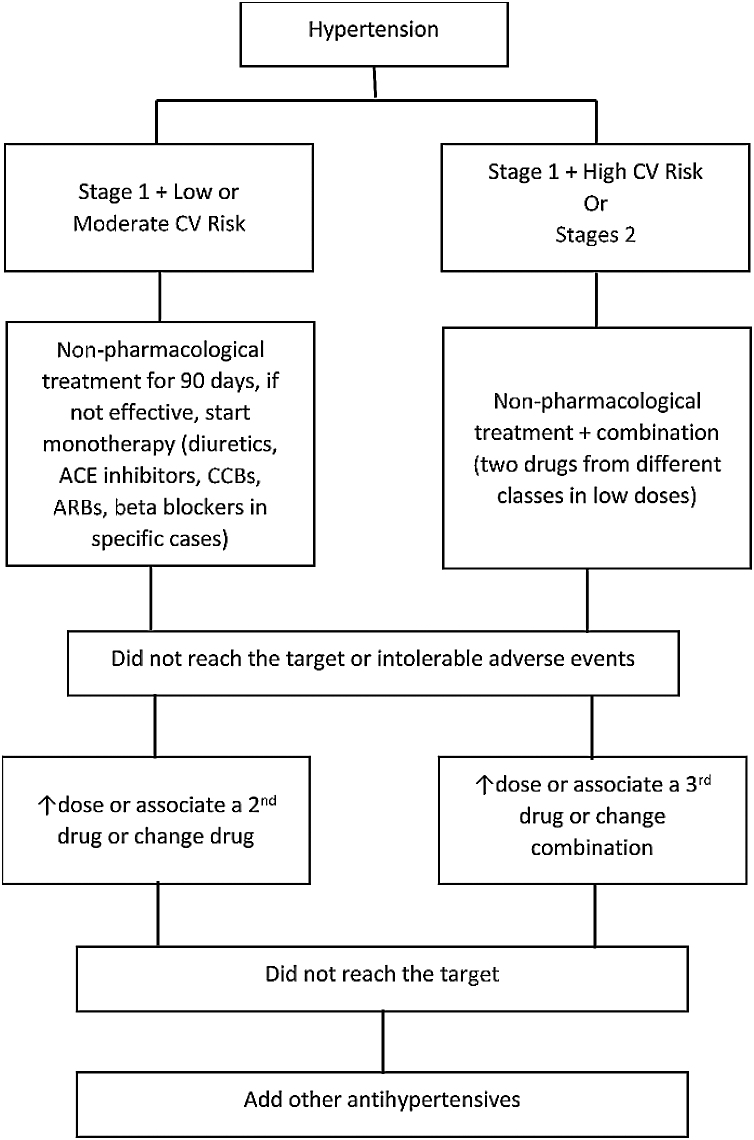
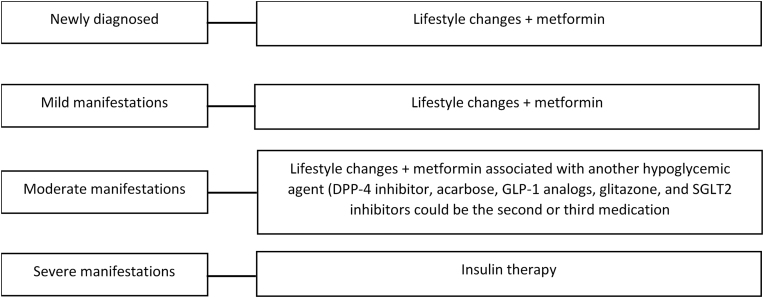
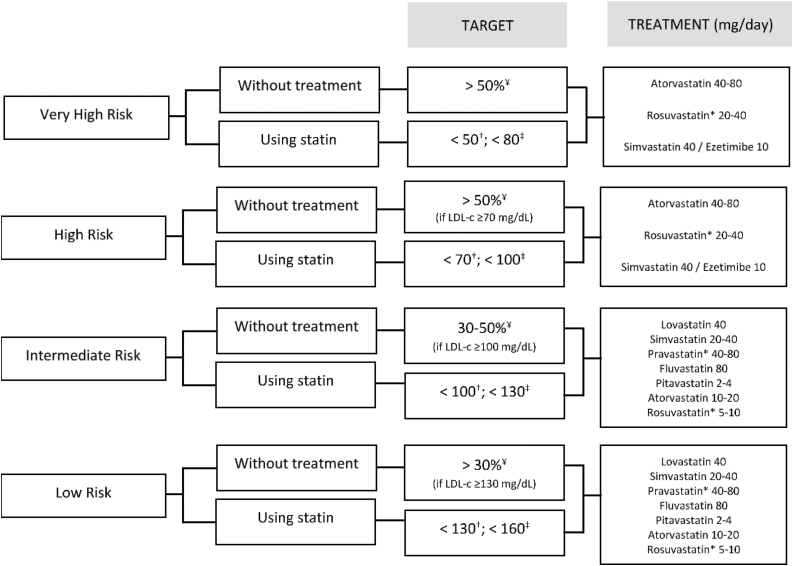
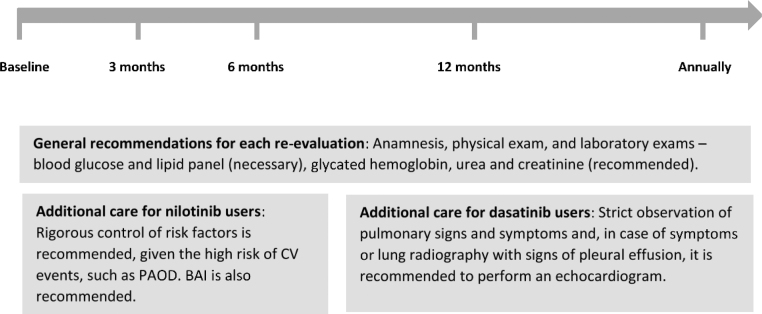
This manuscript summarizes the results of the consensus meeting composed of hematologists and cardiologists to establish recommendations for the prevention and follow-up of cardiovascular (CV) risk in patients with chronic myeloid leukemia (CML) treated with BCR-ABL tyrosine kinase inhibitors (TKIs) from the point of view of clinical practice and from the perspective of hematology consultation. In the first medical appointment, the CV risk factors should be identified to perform the baseline risk stratification, based on the Brazilian Guideline of Dyslipidemia and Atherosclerosis Prevention Update (risk levels: very high, high, intermediate and low). Once stratified, the treatment of the CV risk factors should be administered. If the patient presents risk factors, such as hypertension, diabetes, renal disease, smoking and hypercholesterolemia, the evaluation and initial treatment may be done by the hematologist, being an option the request for evaluation by a specialist. If the patient has a history of previous CV disease, we recommend referral to a specialist. As the CV risk score is dynamic and the control of risk factors can reduce the patient risk, this expert consensus recommends that the re-evaluation of the CV risk after the baseline should be performed at 3 months, 6 months and 12 months. After this period, it should be done annually and, for specific patients, at the clinician's discretion. The evaluation of the baseline CV risk and the safe administration of a TKI allow the patient to benefit from the maximum treatment, avoiding unwanted effects.
Keywords: Cardiovascular diseases; Leukemia, myeloid; Protein kinase inhibitors; Risk factors; Risk management.
Copyright © 2020 Associação Brasileira de Hematologia, Hemoterapia e Terapia Celular. Published by Elsevier España, S.L.U. All rights reserved.
Figures
References
-
- Sociedade Brasileira de Oncologia Clínica (SBOC) Manual de Condutas 2011. Rev Soc Bras Oncol Clin. 2011:589.
-
- Ministério da Saúde (Brasil) Ministério da Saúde; Brasília: 2014. Secretaria de Atenção à Saúde. Protocolos Clínicos e Diretrizes Terapêuticas em Oncologia.
-
- Bower H., Björkholm M., Dickman P.W., Höglund M., Lambert P.C., Andersson T.M.L. Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J Clin Oncol. 2016;34(24):2851–2857. - PubMed
-
- Breccia M., Arboscello E., Bellodi A., Colafigli G., Molica M., Bergamaschi M. Proposal for a tailored stratification at baseline and monitoring of cardiovascular effects during follow-up in chronic phase chronic myeloid leukemia patients treated with nilotinib frontline. Crit Rev Oncol Hematol. 2016;107:190–198. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
