

Association between palliative care and healthcare outcomes among adults with terminal non-cancer illness: population based matched cohort study
- PMID: 32631907
- PMCID: PMC7336238
- DOI: 10.1136/bmj.m2257
Association between palliative care and healthcare outcomes among adults with terminal non-cancer illness: population based matched cohort study
Abstract
Objective: To measure the associations between newly initiated palliative care in the last six months of life, healthcare use, and location of death in adults dying from non-cancer illness, and to compare these associations with those in adults who die from cancer at a population level.
Design: Population based matched cohort study.
Setting: Ontario, Canada between 2010 and 2015.
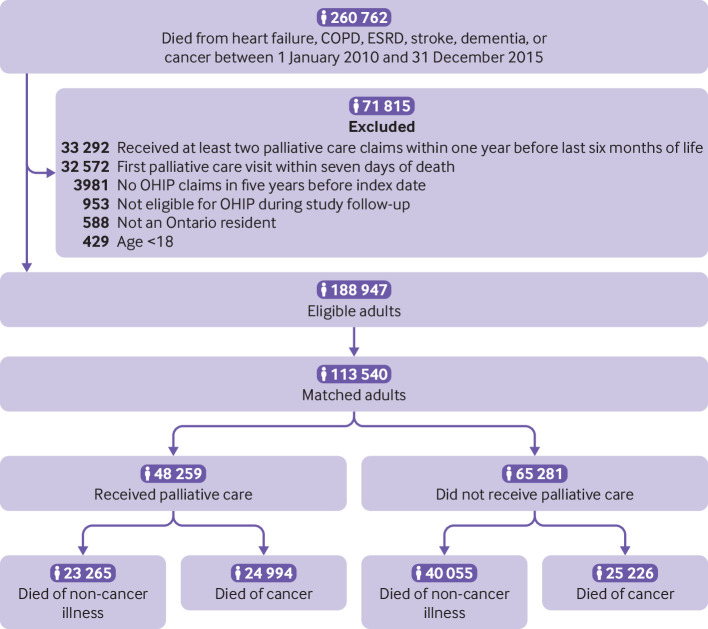
Participants: 113 540 adults dying from cancer and non-cancer illness who were given newly initiated physician delivered palliative care in the last six months of life administered across all healthcare settings. Linked health administrative data were used to directly match patients on cause of death, hospital frailty risk score, presence of metastatic cancer, residential location (according to 1 of 14 local health integration networks that organise all healthcare services in Ontario), and a propensity score to receive palliative care that was derived by using age and sex.
Main outcome measures: Rates of emergency department visits, admissions to hospital, and admissions to the intensive care unit, and odds of death at home versus in hospital after first palliative care visit, adjusted for patient characteristics (such as age, sex, and comorbidities).
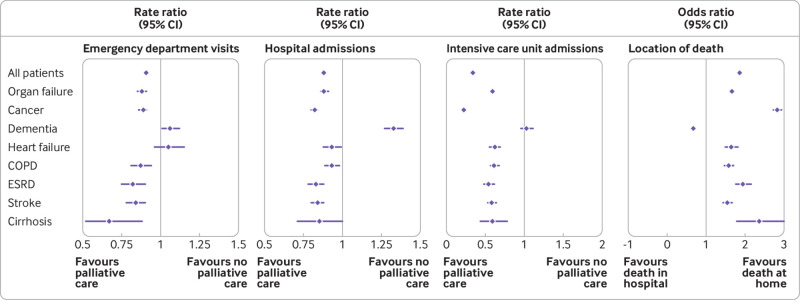
Results: In patients dying from non-cancer illness related to chronic organ failure (such as heart failure, cirrhosis, and stroke), palliative care was associated with reduced rates of emergency department visits (crude rate 1.9 (standard deviation 6.2) v 2.9 (8.7) per person year; adjusted rate ratio 0.88, 95% confidence interval 0.85 to 0.91), admissions to hospital (crude rate 6.1 (standard deviation 10.2) v 8.7 (12.6) per person year; adjusted rate ratio 0.88, 95% confidence interval 0.86 to 0.91), and admissions to the intensive care unit (crude rate 1.4 (standard deviation 5.9) v 2.9 (8.7) per person year; adjusted rate ratio 0.59, 95% confidence interval 0.56 to 0.62) compared with those who did not receive palliative care. Additionally increased odds of dying at home or in a nursing home compared with dying in hospital were found in these patients (n=6936 (49.5%) v n=9526 (39.6%); adjusted odds ratio 1.67, 95% confidence interval 1.60 to 1.74). Overall, in patients dying from dementia, palliative care was associated with increased rates of emergency department visits (crude rate 1.2 (standard deviation 4.9) v 1.3 (5.5) per person year; adjusted rate ratio 1.06, 95% confidence interval 1.01 to 1.12) and admissions to hospital (crude rate 3.6 (standard deviation 8.2) v 2.8 (7.8) per person year; adjusted rate ratio 1.33, 95% confidence interval 1.27 to 1.39), and reduced odds of dying at home or in a nursing home (n=6667 (72.1%) v n=13 384 (83.5%); adjusted odds ratio 0.68, 95% confidence interval 0.64 to 0.73). However, these rates differed depending on whether patients dying with dementia lived in the community or in a nursing home. No association was found between healthcare use and palliative care for patients dying from dementia who lived in the community, and these patients had increased odds of dying at home.
Conclusions: These findings highlight the potential benefits of palliative care in some non-cancer illnesses. Increasing access to palliative care through sustained investment in physician training and current models of collaborative palliative care could improve end-of-life care, which might have important implications for health policy.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Institute for Clinical Evaluative Sciences (ICES) for the submitted work; the analysis was supported by a research grant KLQ and CMB received from the Sinai Health System Research Foundation to perform this work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Palliative care in illnesses other than cancer.BMJ. 2020 Jul 6;370:m2528. doi: 10.1136/bmj.m2528. BMJ. 2020. PMID: 32631929 No abstract available.
-
Initiation of palliative care in the last 6 months of life can reduce the frequency of healthcare use and burdensome interventions for people with both cancer and non-cancer diagnoses.Evid Based Nurs. 2022 Jan;25(1):20. doi: 10.1136/ebnurs-2020-103345. Epub 2020 Nov 17. Evid Based Nurs. 2022. PMID: 33203655 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical