

Minimally invasive right colectomy with transrectal natural orifice extraction: could this be the next step forward?
- PMID: 32632708
- PMCID: PMC7536150
- DOI: 10.1007/s10151-020-02282-x
Minimally invasive right colectomy with transrectal natural orifice extraction: could this be the next step forward?
Abstract
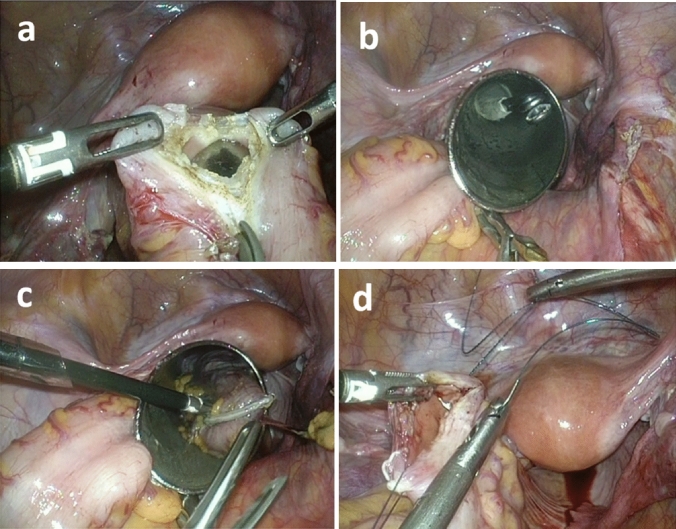
Background: The transvaginal natural orifice specimen extraction (NOSE) approach for right-side colon surgery has been proven to exhibit favorable short-term outcomes. However, thus far, no study has reported the advantages of transrectal NOSE for right-side colon surgery. The aim of this study was to compare the technical feasibility, safety, and short-term outcomes of minimally invasive right hemicolectomy using the transrectal NOSE method and those of conventional mini-laparotomy specimen extraction.
Methods: A study was conducted on consecutive patients who had minimally invasive right hemicolectomy either for malignancy or benign disease at Chang Gung Memorial Hospital, Linkou, Taiwan, between January 2017 and December 2018. The patients were divided into two groups: conventional surgery with specimen extraction using mini-laparotomy and NOSE surgery. Surgical outcomes, including complications, postoperative short-term recovery, and pain intensity, were analyzed.
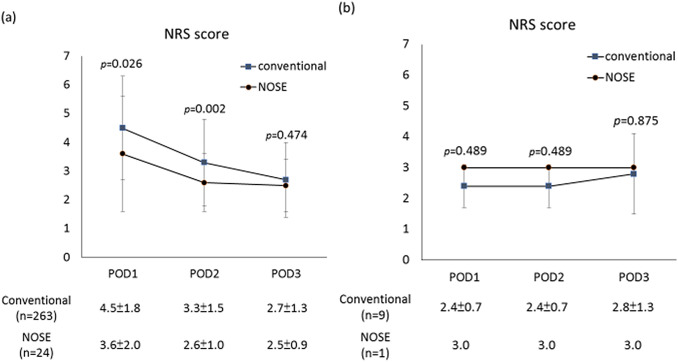
Results: We enrolled 297 patients (151 males, mean age 64.9 ± 12.8 years) who had minimally invasive right hemicolectomy. Of these 297 patients, 272 patients had conventional surgery with specimen extraction through mini-laparotomy and 25 patients had NOSE surgery (23 transrectal, 2 transvaginal). The diagnosis of colon disease did not differ significantly between the conventional and NOSE groups. Postoperative morbidity and mortality rates were comparable. The postoperative hospital stay was significantly (p = 0.004) shorter in the NOSE group (median 5 days, range 3-17 days) than in the conventional group (median 7 days, range 3-45 days). Postoperative pain was significantly (p = 0.026 on postoperative day 1 and p = 0.002 on postoperative day 2) greater in the conventional group than in the NOSE group.
Conclusions: NOSE was associated with acceptable short-term surgical outcomes that were comparable to those of conventional surgery. NOSE results in less postoperative wound pain and a shorter hospital stay than conventional surgery. Larger studies are needed.
Keywords: Laparoscopic surgery; Minimally invasive surgery; Natural orifice specimen extraction (NOSE); Right colectomy; Right hemicolectomy.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Color Study Group COLOR: a randomized clinical trial comparing laparoscopic and open resection for colon cancer. Dig Surg. 2000;17(6):617–622. - PubMed
-
- Clinical Outcomes of Surgical Therapy Study Group A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350(20):2050–2059. - PubMed
-
- Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW, Jr, Hellinger M, Flanagan R, Jr, Peters W, Nelson H. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007;246(4):655–662. - PubMed
-
- Lacy AM, Delgado S, Castells A, Prins HA, Arroyo V, Ibarzabal A, Pique JM. The long-term results of a randomized clinical trial of laparoscopy-assisted versus open surgery for colon cancer. Ann Surg. 2008;248:1–7. - PubMed
-
- Green BL, Marshall HC, Collinson F, Quirke P, Guillou P, Jayne DG, Brown JM. Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer. Br J Surg. 2013;100(1):75–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
