

Cost and effects of integrated care: a systematic literature review and meta-analysis
- PMID: 32632820
- PMCID: PMC7561551
- DOI: 10.1007/s10198-020-01217-5
Cost and effects of integrated care: a systematic literature review and meta-analysis
Abstract
Background: Health and care services are becoming increasingly strained and healthcare authorities worldwide are investing in integrated care in the hope of delivering higher-quality services while containing costs. The cost-effectiveness of integrated care, however, remains unclear. This systematic review and meta-analysis aims to appraise current economic evaluations of integrated care and assesses the impact on outcomes and costs.
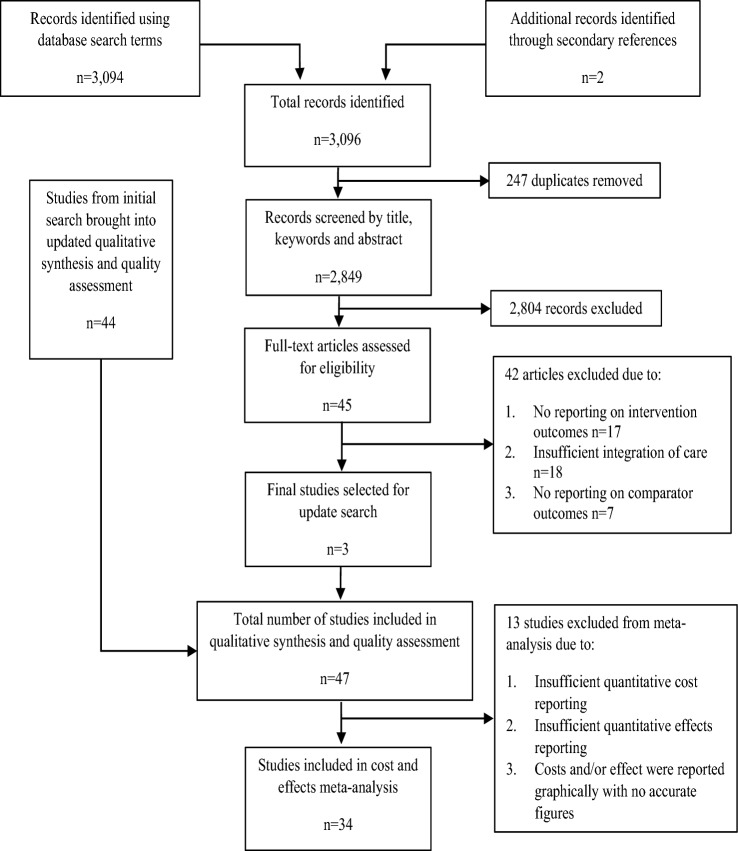
Methods: CINAHL, DARE, EMBASE, Medline/PubMed, NHS EED, OECD Library, Scopus, Web of Science, and WHOLIS databases from inception to 31 December 2019 were searched to identify studies assessing the cost-effectiveness of integrated care. Study quality was assessed using an adapted CHEERS checklist and used as weight in a random-effects meta-analysis to estimate mean cost and mean outcomes of integrated care.
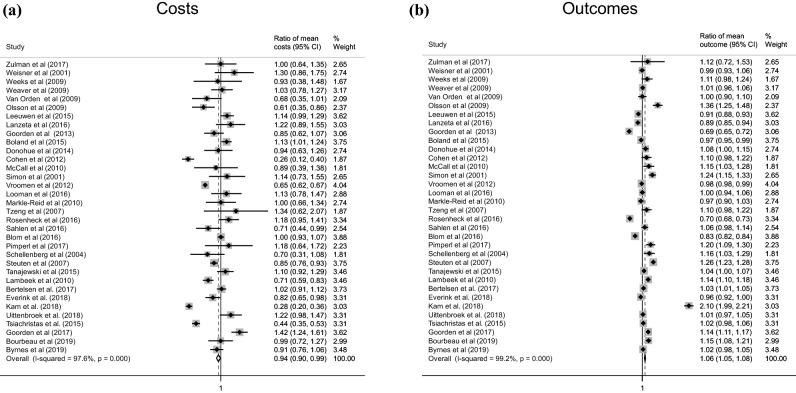
Results: Selected studies achieved a relatively low average quality score of 65.0% (± 18.7%). Overall meta-analyses from 34 studies showed a significant decrease in costs (0.94; CI 0.90-0.99) and a statistically significant improvement in outcomes (1.06; CI 1.05-1.08) associated with integrated care compared to the control. There is substantial heterogeneity in both costs and outcomes across subgroups. Results were significant in studies lasting over 12 months (12 studies), with both a decrease in cost (0.87; CI 0.80-0.94) and improvement in outcomes (1.15; 95% CI 1.11-1.18) for integrated care interventions; whereas, these associations were not significant in studies with follow-up less than a year.
Conclusion: Our findings suggest that integrated care is likely to reduce cost and improve outcome. However, existing evidence varies largely and is of moderate quality. Future economic evaluation should target methodological issues to aid policy decisions with more robust evidence on the cost-effectiveness of integrated care.
Keywords: Cost-effectiveness; Economic evaluation; Integrated care; meta-analysis.
Figures
References
-
- Lorenzoni, L. et al.: Health spending projections to 2030: new results based on a revised OECD methodology, in OECD Health Working Papers. In: Publishing, O. (ed.) Paris (2019)
-
- Improvement, N.: Performance of the NHS provider sector for the year ended 31 March 2018. NHS Improvement, London (2018)
-
- van Vliet, K., Oudenampsen, D.: Integrated care in the Netherlands. Verwey-Jonker Instituut. (2004)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
