

Putative Cut-Points in Sarcopenia Components and Incident Adverse Health Outcomes: An SDOC Analysis
- PMID: 32633824
- PMCID: PMC7508260
- DOI: 10.1111/jgs.16517
Putative Cut-Points in Sarcopenia Components and Incident Adverse Health Outcomes: An SDOC Analysis
Abstract
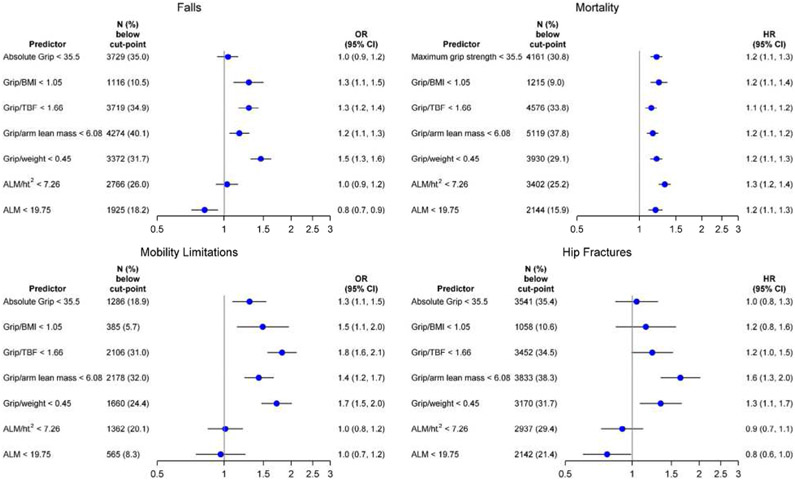
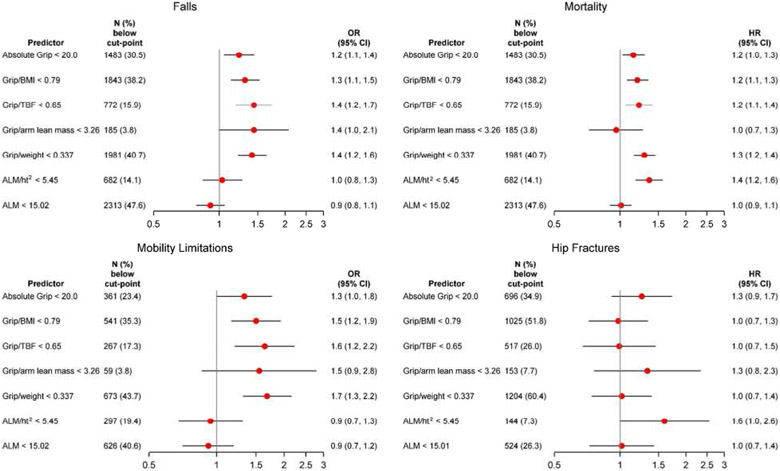
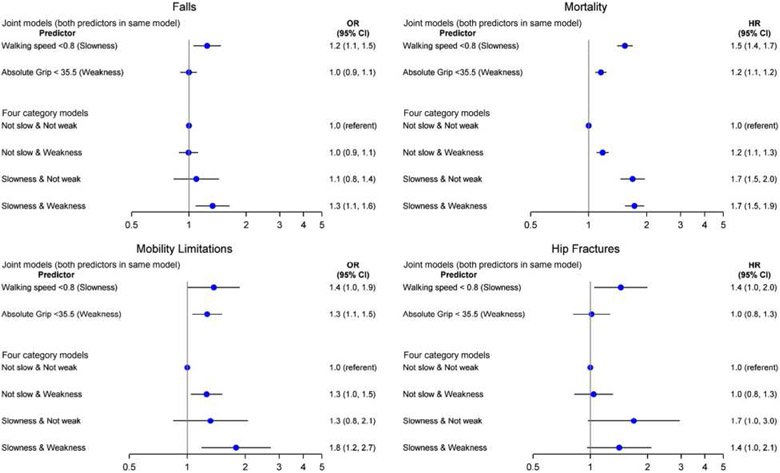
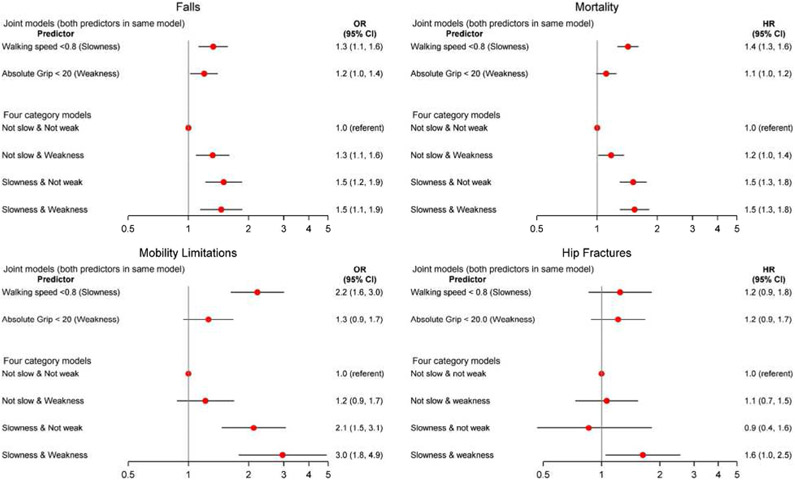
Objectives: Analyses performed by the Sarcopenia Definitions and Outcomes Consortium (SDOC) identified cut-points in several metrics of grip strength for consideration in a definition of sarcopenia. We describe the associations between the SDOC-identified metrics of low grip strength (absolute or standardized to body size/composition); low dual-energy x-ray absorptiometry (DXA) lean mass as previously defined in the literature (appendicular lean mass [ALM]/ht2 ); and slowness (walking speed <.8 m/s) with subsequent adverse outcomes (falls, hip fractures, mobility limitation, and mortality).
Design: Individual-level, sex-stratified pooled analysis. We calculated odds ratios (ORs) or hazard ratios (HRs) for incident falls, mobility limitation, hip fractures, and mortality. Follow-up time ranged from 1 year for falls to 8.8 ± 2.3 years for mortality.
Setting: Eight prospective observational cohort studies.
Participants: A total of 13,421 community-dwelling men and 4,828 community-dwelling women. MEASUREMENTS Grip strength by hand dynamometry, gait speed, and lean mass by DXA.
Results: Low grip strength (absolute or standardized to body size/composition) was associated with incident outcomes, usually independently of slowness, in both men and women. ORs and HRs generally ranged from 1.2 to 3.0 for those below vs above the cut-point. DXA lean mass was not consistently associated with these outcomes. When considered together, those who had both muscle weakness by absolute grip strength (<35.5 kg in men and <20 kg in women) and slowness were consistently more likely to have a fall, hip fracture, mobility limitation, or die than those without either slowness or muscle weakness.
Conclusion: Older men and women with both muscle weakness and slowness have a higher likelihood of adverse health outcomes. These results support the inclusion of grip strength and walking speed as components in a summary definition of sarcopenia. J Am Geriatr Soc 68:1429-1437, 2020.
Keywords: gait speed; grip strength; hip fracture; mobility limitation; sarcopenia.
© 2020 The American Geriatrics Society.
Figures
Comment in
-
Role of Sarcopenia Definition and Diagnosis in Clinical Care: Moving from Risk Assessment to Mechanism-Guided Interventions.J Am Geriatr Soc. 2020 Jul;68(7):1406-1409. doi: 10.1111/jgs.16575. Epub 2020 Jul 7. J Am Geriatr Soc. 2020. PMID: 32633862 No abstract available.
References
-
- Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101. - PubMed
Publication types
MeSH terms
Grants and funding
- S3486/CC/CDC HHS/United States
- N01HC85081/HL/NHLBI NIH HHS/United States
- N01HC85083/HL/NHLBI NIH HHS/United States
- 5-P60-AR30701/AR/NIAMS NIH HHS/United States
- K23 AG050260/AG/NIA NIH HHS/United States
- N01AG62106/AG/NIA NIH HHS/United States
- N01-HC-25195/HL/NHLBI NIH HHS/United States
- N01AG62101/AG/NIA NIH HHS/United States
- R01AG023629/AG/NIA NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- U01HL130114/HL/NHLBI NIH HHS/United States
- N01AG62103/AG/NIA NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- UL1 TR000128/TR/NCATS NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- U01HL080295/HL/NHLBI NIH HHS/United States
- P30 AG024827/AG/NIA NIH HHS/United States
- S043, S1734/CC/CDC HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- P30 AG031679/AG/NIA NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- N01HC55222/HL/NHLBI NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- P30 AG028747/AG/NIA NIH HHS/United States
- N01HC85082/HL/NHLBI NIH HHS/United States
- AG51421/AG/NIA NIH HHS/United States
- R01 AG054366/AG/NIA NIH HHS/United States
- U01 AG051421/AG/NIA NIH HHS/United States
- R01 AR35582/NH/NIH HHS/United States
- R01 AR 41398/NH/NIH HHS/United States
- R01 AR049439-01A1/NH/NIH HHS/United States
- P30 AG028740/AG/NIA NIH HHS/United States
- R01 AG027576/AG/NIA NIH HHS/United States
- R01 AG005394/AG/NIA NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- R01 AG048069/AG/NIA NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- R01AR35584/NH/NIH HHS/United States
- R01 AR35583/NH/NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- N01HC85080/HL/NHLBI NIH HHS/United States
- K01 AG057726/AG/NIA NIH HHS/United States
- R01 AG027574/AG/NIA NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
- R01AR057118/NH/NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- U24AG051129/AG/NIA NIH HHS/United States
- 5 P60 AR49465-03/AR/NIAMS NIH HHS/United States
- N01HC85086/HL/NHLBI NIH HHS/United States
- N01HC85079/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
