

All-Cause and Cardiovascular Disease Mortality Among Breast Cancer Survivors in CLUE II, a Long-Standing Community-Based Cohort
- PMID: 32634223
- PMCID: PMC7850550
- DOI: 10.1093/jnci/djaa096
All-Cause and Cardiovascular Disease Mortality Among Breast Cancer Survivors in CLUE II, a Long-Standing Community-Based Cohort
Abstract
Background: There is growing evidence that breast cancer survivors have higher cardiovascular disease (CVD) mortality relative to the general population. Information on temporal patterns for all-cause and CVD mortality among breast cancer survivors relative to cancer-free women is limited.
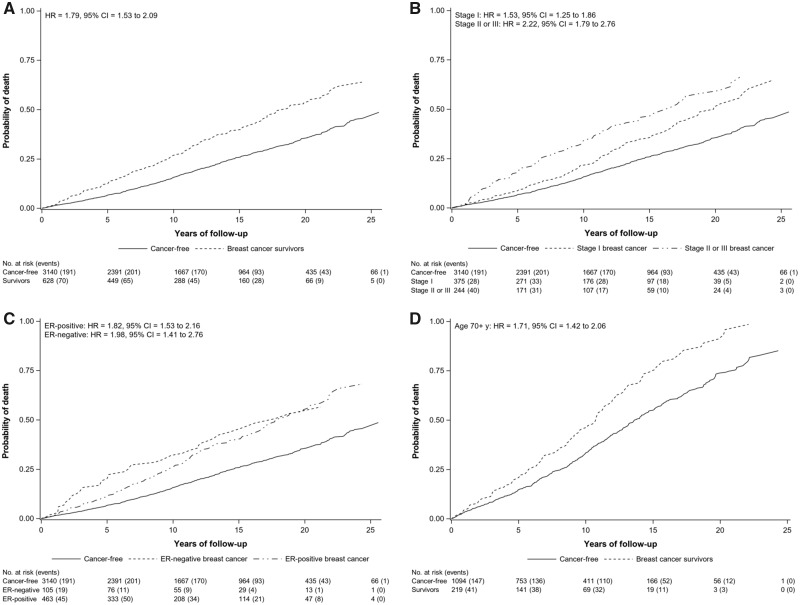
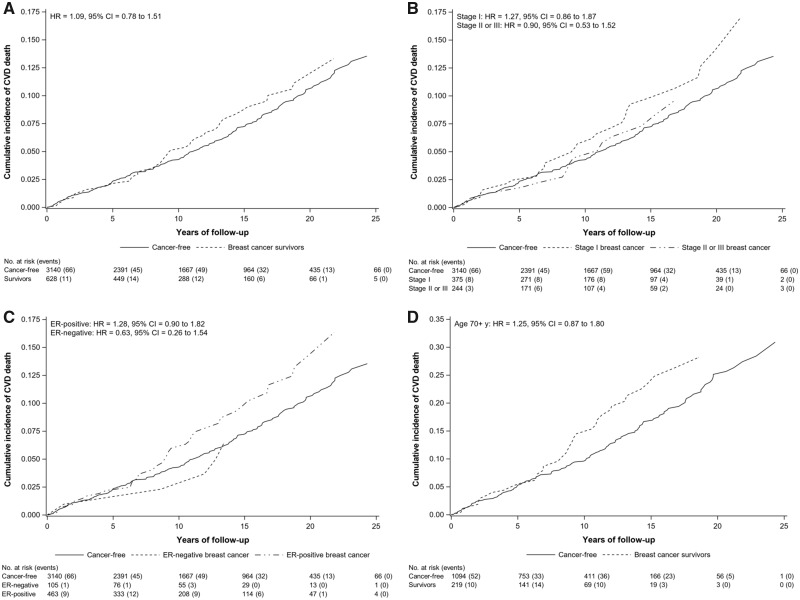
Methods: All-cause and CVD-related mortality were compared in 628 women with breast cancer and 3140 age-matched cancer-free women within CLUE II, a prospective cohort. We calculated adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) using Cox proportional hazards regression for all-cause mortality, and Fine and Gray models for CVD-related mortality to account for competing risks.
Results: Over 25 years of follow-up, 916 deaths occurred (249 CVD related). Breast cancer survivors had an overall higher risk of dying compared with cancer-free women (HR = 1.79, 95% CI = 1.53 to 2.09) irrespective of time since diagnosis, tumor stage, estrogen receptor status, and older age at diagnosis (≥70 years). Risk of death was greatest among older survivors at more than 15 years after diagnosis (HR = 2.69, 95% CI = 1.59 to 4.55). CVD (69.1% ischemic heart disease) was the leading cause of death among cancer-free women and the second among survivors. Survivors had an increase in CVD-related deaths compared with cancer-free women beginning at 8 years after diagnosis (HR = 1.65, 95% CI = 1.00 to 2.73), with the highest risk among older survivors (HR = 2.24, 95% CI = 1.29 to 3.88) and after estrogen receptor-positive disease (HR = 1.85, 95% CI = 1.06 to 3.20).
Conclusions: Breast cancer survivors continue to have an elevated mortality compared with the general population for many years after diagnosis. Preventing cardiac deaths, particularly among older breast cancer patients, could lead to reductions in mortality.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Cardiovascular Disease in Breast Cancer Survivors: An Important Topic in Breast Cancer Survivorship.J Natl Cancer Inst. 2021 Feb 1;113(2):105-106. doi: 10.1093/jnci/djaa097. J Natl Cancer Inst. 2021. PMID: 32634213 Free PMC article. No abstract available.
References
-
- Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin 2019;69(5):363–385. - PubMed
-
- American Cancer Society. Breast Cancer Facts & Figures 2019-2020. Atlanta, GA: American Cancer Society, Inc; 2019.
-
- Schairer C, Mink PJ, Carroll L, et al.Probabilities of death from breast cancer and other causes among female breast cancer patients. J Natl Cancer Inst. 2004;96(17):1311–1321. - PubMed
-
- Abdel-Qadir H, Austin PC, Lee DS, et al.A population-based study of cardiovascular mortality following early-stage breast cancer. JAMA Cardiol. 2017;2(1):88–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
