

Longitudinal Analysis of Depression and Anxiety Symptoms as Independent Predictors of Neurocognitive Function in Primary Brain Tumor Patients
- PMID: 32634542
- PMCID: PMC7680441
- DOI: 10.1016/j.ijrobp.2020.07.002
Longitudinal Analysis of Depression and Anxiety Symptoms as Independent Predictors of Neurocognitive Function in Primary Brain Tumor Patients
Abstract
Purpose: Primary brain tumor patients are vulnerable to depression and anxiety symptoms, which may affect their neurocognitive functioning. We performed a prospective longitudinal analysis to examine the association between depression and anxiety symptoms and domain-specific neurocognitive functioning in primary brain tumor patients receiving radiation therapy (RT).
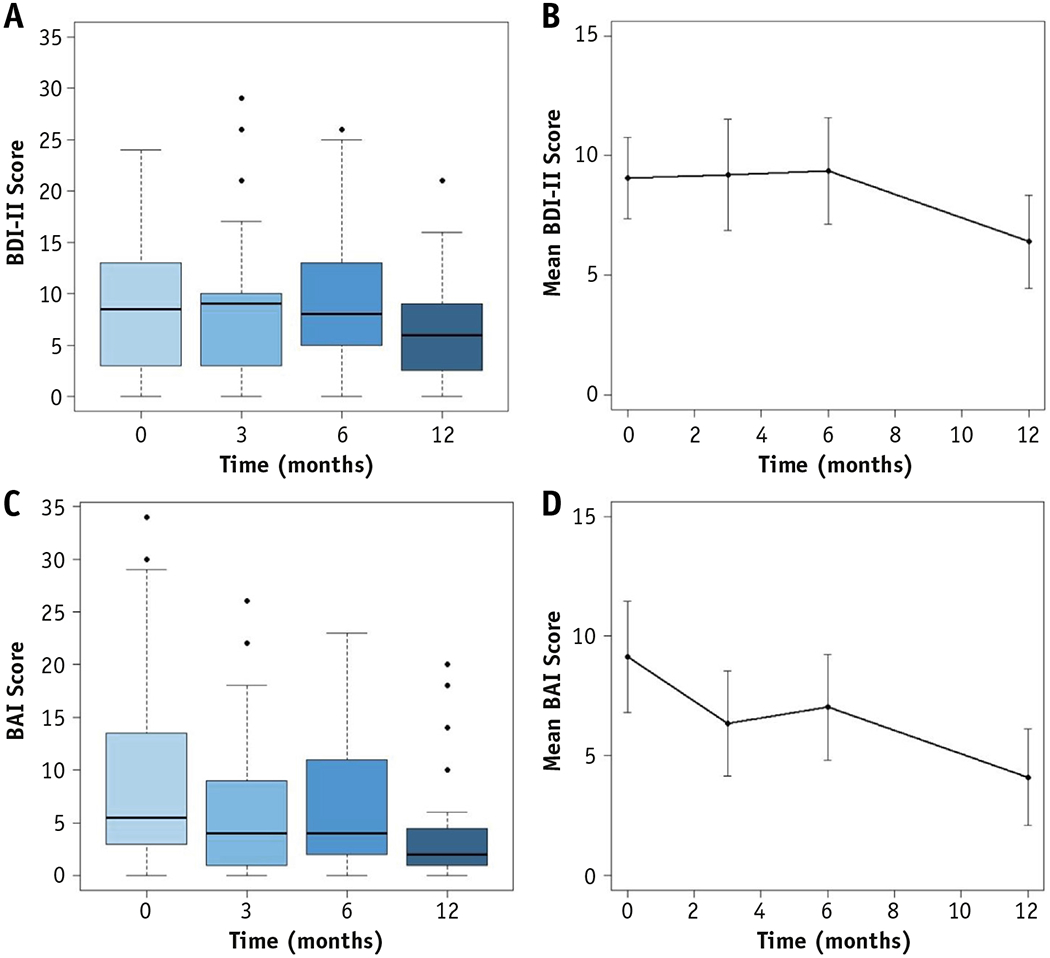
Methods and materials: On a prospective trial, 54 primary brain tumor patients receiving RT underwent comprehensive neurocognitive evaluation at baseline (pre-RT), and 3, 6, and 12 months post-RT. Neurocognitive assessments measured attention/processing speed, verbal and visuospatial memory, and executive functioning, including Delis-Kaplan Executive Function System Trail-Making Test (DKEFS-TMT), DKEFS Verbal Fluency, and Brief Visuospatial Memory Test-Revised. Depression and anxiety symptoms were also assessed at each time point with Beck Depression and Anxiety Inventories (BDI-II and BAI), respectively. Higher scores reflect more numerous or severe depression or anxiety symptoms. Univariable and multivariable linear mixed-effects models assessed associations between BDI-II and BAI scores and domain-specific neurocognitive scores over time, controlling for pre-existing depression or anxiety disorders and other patient, tumor, and treatment characteristics.
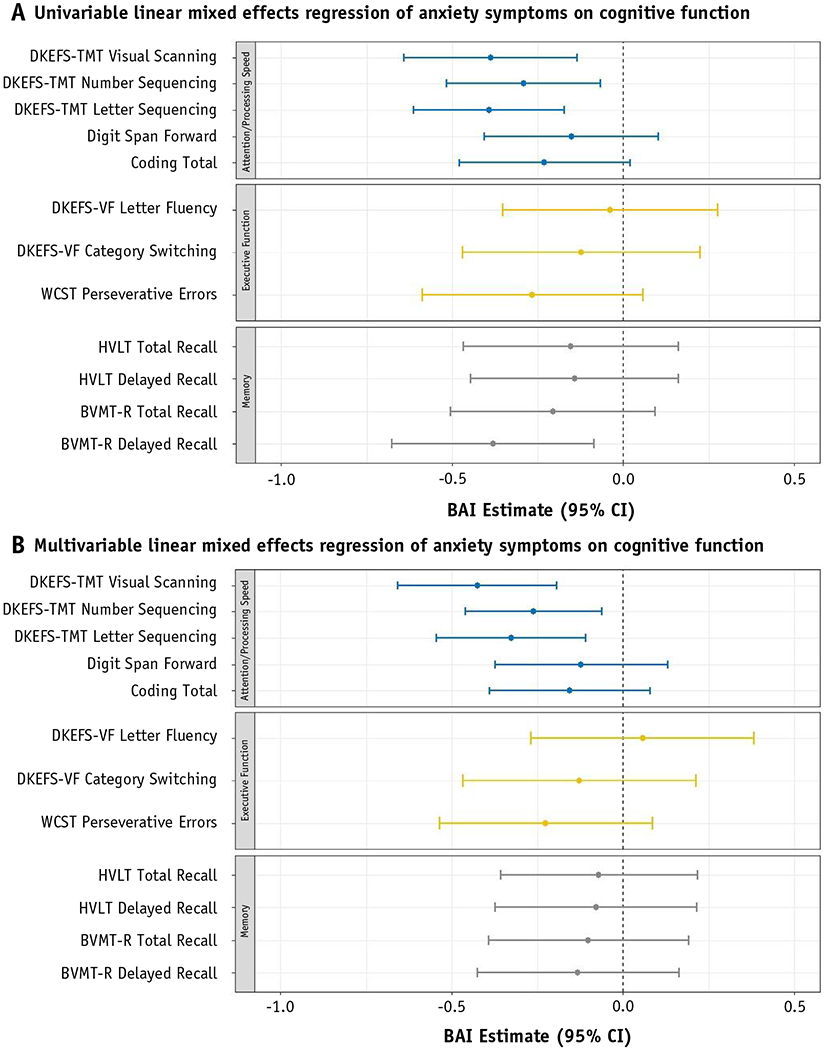
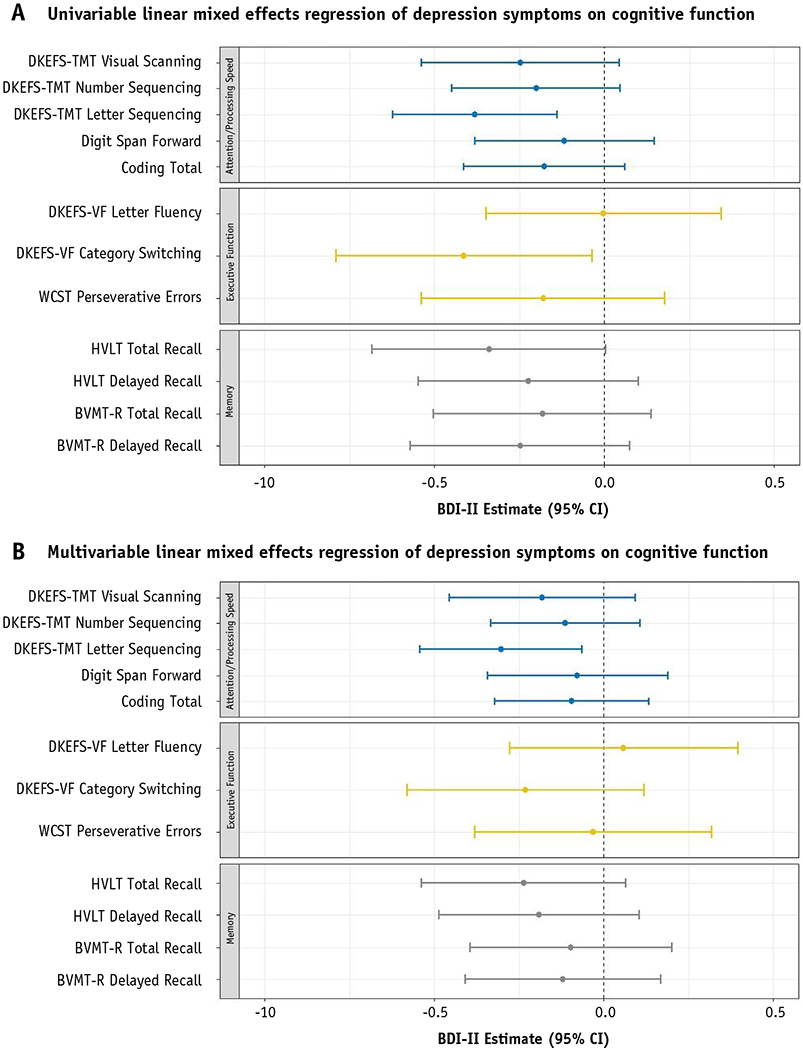
Results: Higher BAI scores were associated with worse attention and processing speed in univariable analyses: DKEFS-TMT visual scanning (P = .003), number sequencing (P = .011), and letter sequencing (P <.001). On multivariable analyses, these associations remained significant (all P ≤ .01). Higher BDI-II scores were also associated with poorer attention/processing speed (DKEFS-TMT Letter Sequencing) in univariable (P = .002) and multivariable (P = .013) models. Higher BAI scores were associated with worse visuospatial memory (Brief Visuospatial Memory Test-Revised Delayed Recall) on univariable (P = .012) but not multivariable analyses (P = .383). Similarly, higher BDI-II scores were associated with poorer executive functioning (DKEFS Verbal Fluency Category Switching) on univariable (P = .031) but not multivariable analyses (P = .198).
Conclusions: Among primary brain tumor patients receiving RT, increased depression and anxiety were independently associated with worsened neurocognition, particularly in attention/processing speed. Depression and anxiety symptoms should be controlled for in prospective clinical trials and managed in the clinical setting to optimize neurocognitive functioning.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
Comment in
-
In Regard to Tibbs et al.Int J Radiat Oncol Biol Phys. 2021 Jun 1;110(2):611-612. doi: 10.1016/j.ijrobp.2020.12.059. Int J Radiat Oncol Biol Phys. 2021. PMID: 33989580 No abstract available.
-
In Reply to Bunevicius et al.Int J Radiat Oncol Biol Phys. 2021 Jun 1;110(2):612. doi: 10.1016/j.ijrobp.2020.12.058. Int J Radiat Oncol Biol Phys. 2021. PMID: 33989581 No abstract available.
References
-
- Litofsky SN, Resnick AG. The relationships between depression and brain tumors. J Neurooncol 2009;94:153–161. - PubMed
-
- Fox SW, Lyon D, Farace E. Symptom clusters in patients with high-grade glioma: Clinical scholarship. J Nurs Scholarsh 2007;39:61–67. - PubMed
-
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment. Arch Intern Med 2000; 160:2101. - PubMed
-
- Bortolato B, Hyphantis TN, Valpione S, et al. Depression in cancer: The many biobehavioral pathways driving tumor progression. Cancer Treat Rev 2017;52:58–70. - PubMed
