

The Use of 13C-Urea Breath Test for Non-Invasive Diagnosis of Helicobacter pylori Infection in Comparison to Endoscopy and Stool Antigen Test
- PMID: 32635179
- PMCID: PMC7400053
- DOI: 10.3390/diagnostics10070448
The Use of 13C-Urea Breath Test for Non-Invasive Diagnosis of Helicobacter pylori Infection in Comparison to Endoscopy and Stool Antigen Test
Abstract
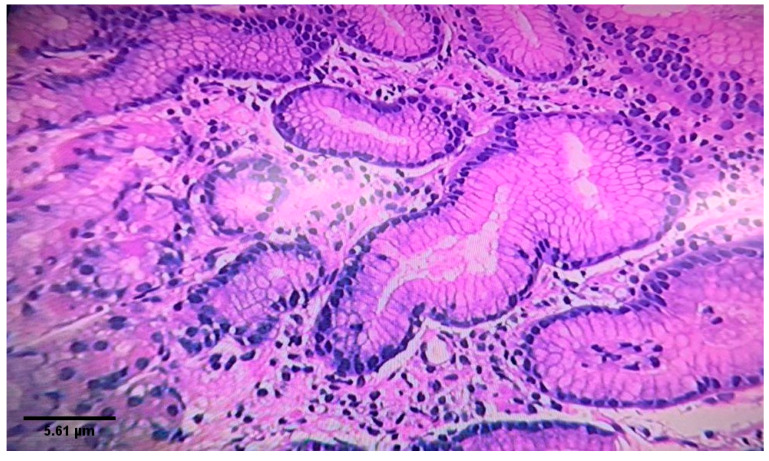
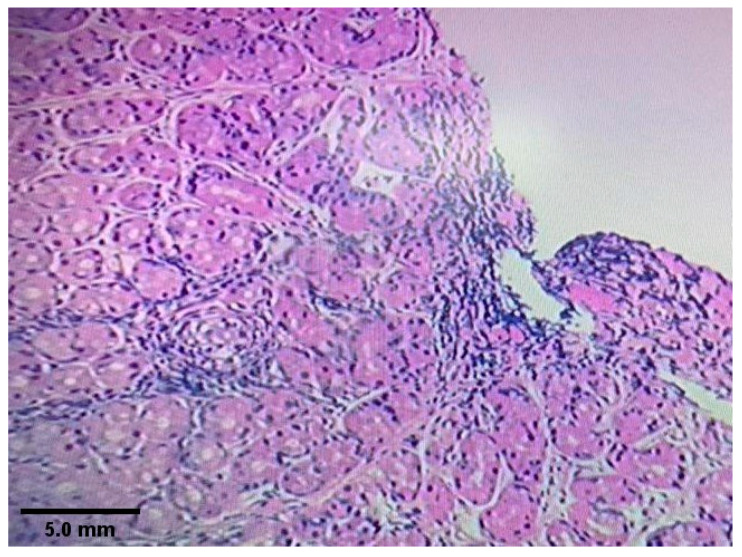
Helicobacter pylori (H. pylori) can cause gastritis, peptic ulcer diseases and gastric carcinoma. Endoscopy as the gold standard method of diagnosis is an invasive procedure that might not be suitable in all scenarios. Therefore, this first study in Jordan aimed to assess the non-invasive 13C urea breath test (UBT) and stool antigen test for diagnosis of H. pylori infection and the successfulness of eradication therapy as alternatives for endoscopy. Hence, a total of 30 patients attending the endoscopy units at Alkarak teaching hospital were asked to complete a questionnaire with demographic and clinical data. They were then tested for H. pylori using 13C UBT and H. pylori stool antigen before having endoscopy. Another 30 patients who were positive for H. pylori by endoscopy were tested using both tests 6 weeks post eradication therapy. Results showed that the rate of H. pylori detection using endoscopy was 56.7% (17/30). Heartburns (82.3%, p value = 0.019), epigastric pain (88.2%, p value = 0.007) and vomiting (70.5%, p value = 0.02) were the most significant symptoms. Family history of peptic ulcer diseases was significantly associated with an increased risk for having a H. pylori positive result (p value = 0.02). Compared to endoscopy, the sensitivity of 13C UBT for the diagnosis of H. pylori was 94.1% (16/17), while it was 76.5% (13/17) for the stool antigen test. The specificity of both tests was equal (76.9%). However, the positive predictive and negative predictive values (84.2% and 90.9%) for 13C UBT were higher than those (81.3% and 71.4%) for the stool antigen test. The accuracy of 13C UBT was 86.7% compared to 76.7% for the stool antigen test. There was an 87% agreement (20 patients out of 23) between both tests when used to assess success of the eradication therapy. In conclusion, the 13C UBT was found to be more sensitive and accurate than the stool antigen test when used for diagnosis; furthermore, it has a comparable outcome to the stool antigen test in assessing the successfulness of the eradication treatment.
Keywords: 13C urea breath test; Helicobacter pylori; endoscopy; sensitivity; stool antigen test.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
