

Rapid Depletion of Subcutaneous Adipose Tissue during Sorafenib Treatment Predicts Poor Survival in Patients with Hepatocellular Carcinoma
- PMID: 32635536
- PMCID: PMC7407859
- DOI: 10.3390/cancers12071795
Rapid Depletion of Subcutaneous Adipose Tissue during Sorafenib Treatment Predicts Poor Survival in Patients with Hepatocellular Carcinoma
Abstract
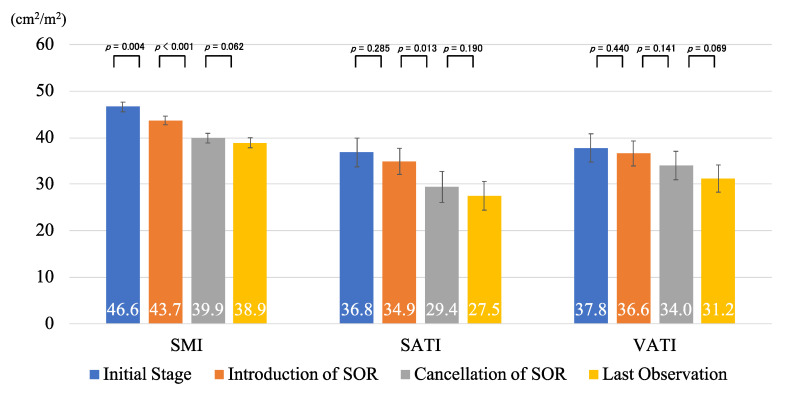
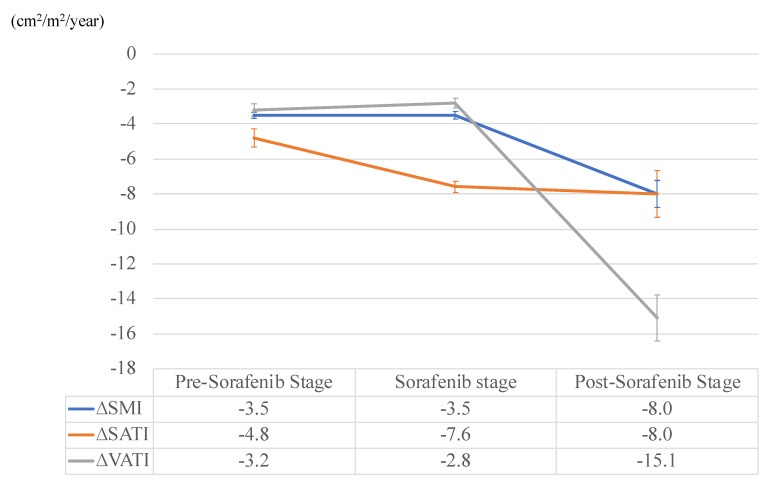
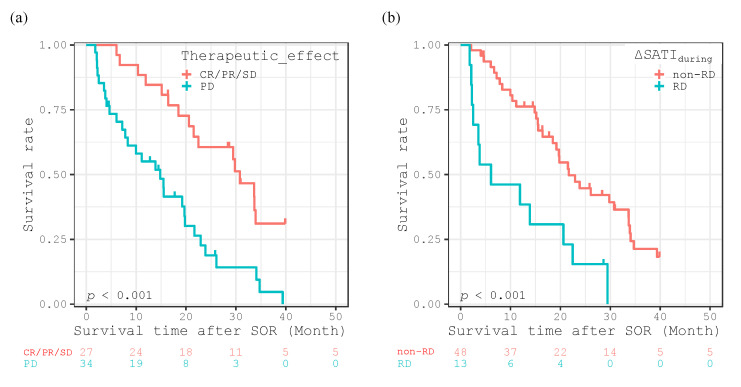
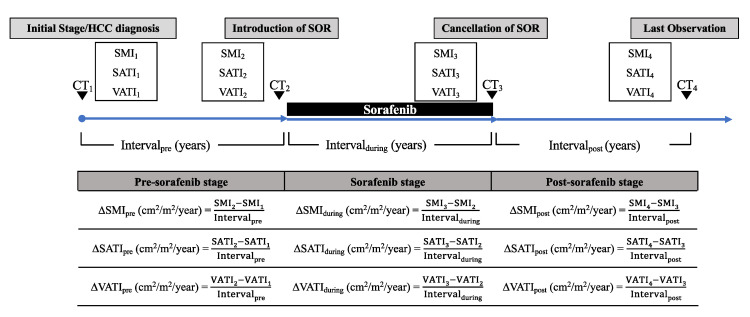
The aim of this study was to assess the annualized changes in body composition, including skeletal muscle, subcutaneous adipose tissue (SAT), and visceral adipose tissue (VAT) before, during, and after sorafenib treatment in patients with hepatocellular carcinoma (HCC). This retrospective study evaluated 61 HCC patients treated with sorafenib. Annualized changes (Δ; cm2/m2/year) in skeletal muscle index (SMI), SAT index (SATI), and VAT index (VATI), which were defined as the cross-sectional areas (cm2) of those areas on computed tomography normalized by the square of one's height (m2), before (pre), during (during), and after (post) sorafenib treatment, were calculated. Patients within the 20th percentile cutoffs for these indices were classified into the rapid depletion group and the effects of these values on survival were analyzed using the Kaplan-Meier analysis and Cox proportional-hazards model. Annualized depletion rates of SMI (ΔSMIpre: -3.5, ΔSMIduring: -3.5, ΔSMIpost: -8.0) and VATI (ΔVATIpre: -3.2, ΔVATIduring: -2.8, ΔVATIpost: -15.1) accelerated after the cancellation of sorafenib, whereas that of SATI (ΔSATIpre: -4.8, ΔSATIduring; -7.6, ΔSATIpost; -8.0) had already accelerated during sorafenib treatment. Patients with rapid depletion of ΔSATIduring experienced significantly worse survival rates (p < 0.001), and it was an independent predictor of survival (p = 0.009), together with therapeutic effect (p < 0.001). Rapid depletion of SAT during sorafenib treatment can be used to predict survival in patients with HCC.
Keywords: body composition; hepatocellular carcinoma; prognostic factor; skeletal muscle; sorafenib; subcutaneous fat mass.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
