

Living Donor Kidney Transplantation Improves Graft and Recipient Survival in Patients with Multiple Kidney Transplants
- PMID: 32635614
- PMCID: PMC7408952
- DOI: 10.3390/jcm9072118
Living Donor Kidney Transplantation Improves Graft and Recipient Survival in Patients with Multiple Kidney Transplants
Abstract
Background: Failed kidney transplant recipients benefit from a new graft as the general incident dialysis population, although additional challenges in the management of these patients are often limiting the long-term outcomes. Previously failed grafts, a long history of comorbidities, side effects of long-term immunosuppression and previous surgical interventions are common characteristics in the repeated kidney transplantation population, leading to significant complex immunological and technical aspects and often compromising the short- and long-term results. Although recipients' factors are acknowledged to represent one of the main determinants for graft and patient survival, there is increasing interest in expanding the donor's pool safely, particularly for high-risk candidates. The role of living kidney donation in this peculiar context of repeated kidney transplantation has not been assessed thoroughly. The aim of the present study is to analyse the effects of a high-quality graft, such as the one retrieved from living kidney donors, in the repeated kidney transplant population context.
Methods: Retrospective analysis of the outcomes of the repeated kidney transplant population at our institution from 1968 to 2019. Data were extracted from a prospectively maintained database and stratified according to the number of transplants: 1st, 2nd or 3rd+. The main outcomes were graft and patient survivals, recorded from time of transplant to graft failure (return to dialysis) and censored at patient death with a functioning graft. Duration of renal replacement therapy was expressed as cumulative time per month. A multivariate analysis considering death-censored graft survival, decade of transplantation, recipient age, donor age, living donor, transplant number, ischaemic time, time on renal replacement therapy prior to transplant and HLA mismatch at HLA-A, -B and -DR was conducted. In the multivariate analysis of recipient survival, diabetic nephropathy as primary renal disease was also included.
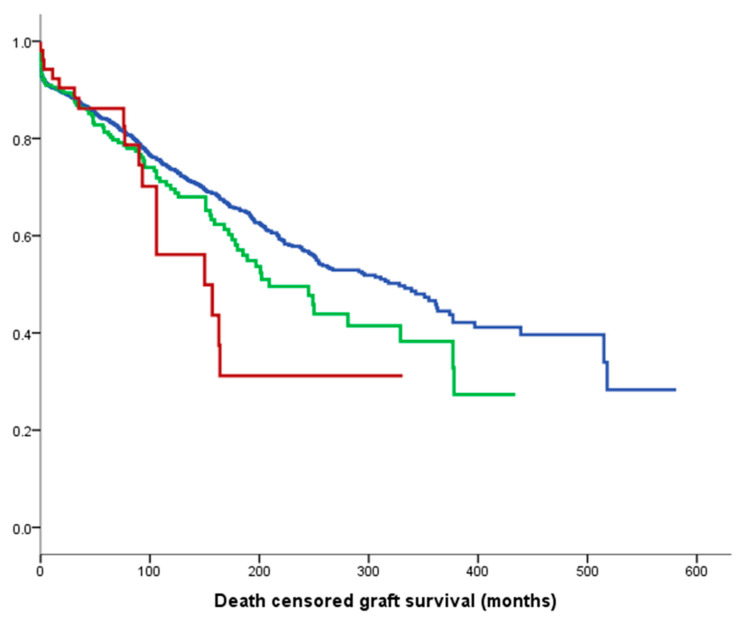
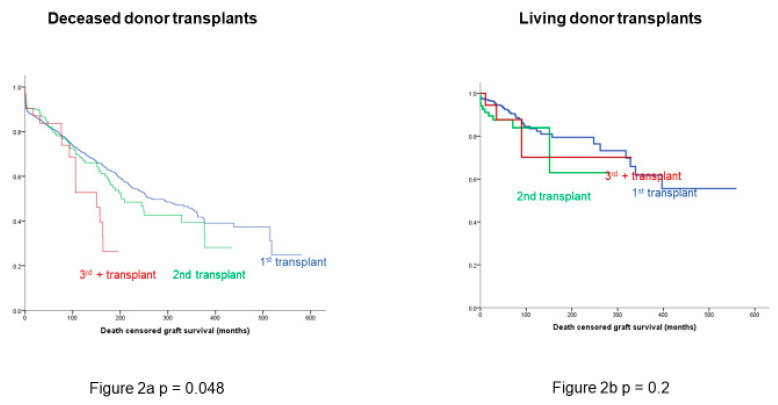
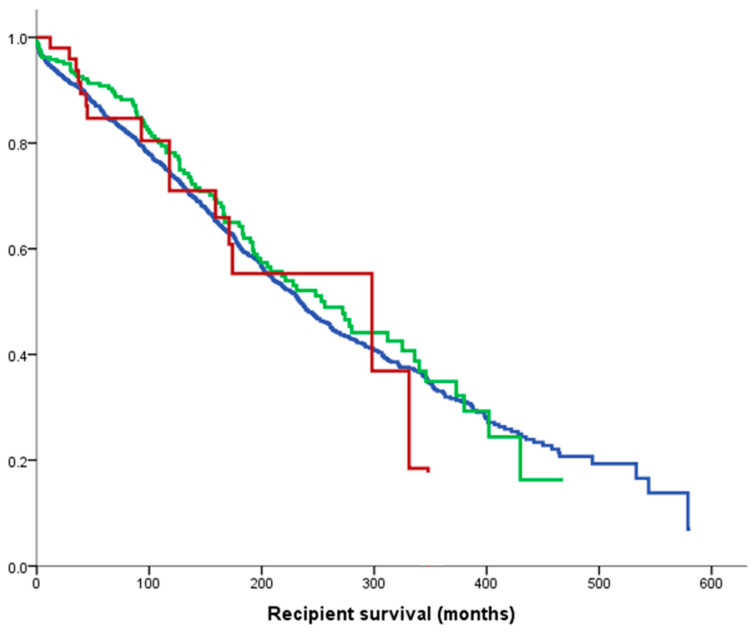
Results: A total of 2395 kidney transplant recipients were analysed: 2062 (83.8%) with the 1st kidney transplant, 279 (11.3%) with the 2nd graft, 46 (2.2%) with the 3rd+. Mean age of 1st kidney transplant recipients was 43.6 ± 16.3 years, versus 39.9 ± 14.4 for 2nd and 41.4 ± 11.5 for 3rd+ (p < 0.001). Aside from being younger, repeated kidney transplant patients were also more often males (p = 0.006), with a longer time spent on renal replacement therapy (p < 0.0001) and a higher degree of sensitisation, expressed as calculated reaction frequency (p < 0.001). There was also an association between multiple kidney transplants and better HLA match at transplantation (p < 0.0001). A difference in death-censored graft survival by number of transplants was seen, with a median graft survival of 328 months for recipients of the 1st transplant, 209 months for the 2nd and 150 months for the 3rd+ (p = 0.038). The same difference was seen in deceased donor kidneys (p = 0.048), but not in grafts from living donors (p = 0.2). Patient survival was comparable between the three groups (p = 0.59).
Conclusions: In the attempt to expand the organ donor pool, particular attention should be reserved to high complex recipients, such as the repeated kidney transplant population. In this peculiar context, the quality of the donor has been shown to represent a main determinant for graft survival-in fact, kidney retrieved from living donors provide comparable outcomes to those from single-graft recipients.
Keywords: graft survival; living donation; patient survival; pre-emptive transplantation; prolonged ischaemic time; repeated kidney transplantation.
Conflict of interest statement
The authors declare no conflict of interest with relevance to the present study.
Figures
References
-
- U.S. Renal Data System, USRDS 2009 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD, USA: 2009.
-
- U.S. Renal Data System, USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD, USA: 2010.
-
- Mehrabi S., Sohn S., Li D., Pankratz J.J., Therneau T., Sauver J.L.S., Liu H., Palakal M. Temporal pattern and association discovery of diagnosis codes using deep learning; Proceedings of the 2015 International Conference on Healthcare Informatics; Richardson, TX, USA. 21–23 October 2015; pp. 408–416.
LinkOut - more resources
Full Text Sources
Research Materials
