

Racial Differences in Diuretic Efficiency, Plasma Renin, and Rehospitalization in Subjects With Acute Heart Failure
- PMID: 32635768
- PMCID: PMC7474850
- DOI: 10.1161/CIRCHEARTFAILURE.119.006827
Racial Differences in Diuretic Efficiency, Plasma Renin, and Rehospitalization in Subjects With Acute Heart Failure
Abstract
Background: Black patients have higher rates of hospitalization for acute heart failure than other race/ethnic groups. We sought to determine whether diuretic efficiency is associated with racial differences in risk for rehospitalization after acute heart failure.
Methods: A post hoc analysis was performed on 721 subjects (age, 68±13 years; 22% black) enrolled in 3 acute heart failure clinical trials: ROSE-AHF (Renal Optimization Strategies Evaluation in Acute Heart Failure), DOSE-AHF (Diuretic Optimization Strategy Evaluation in Acute Decompensated Heart Failure), and CARRESS-HF (Cardiorenal Rescue Study in Acute Decompensated Heart Failure). Repeated-measures ANOVA was used to test for a race×time effect on measures of decongestion. Diuretic efficiency was calculated as net fluid balance per total furosemide equivalents. In a subset of subjects, Cox regression was used to examine the association between race and rehospitalization according to plasma renin activity (PRA).
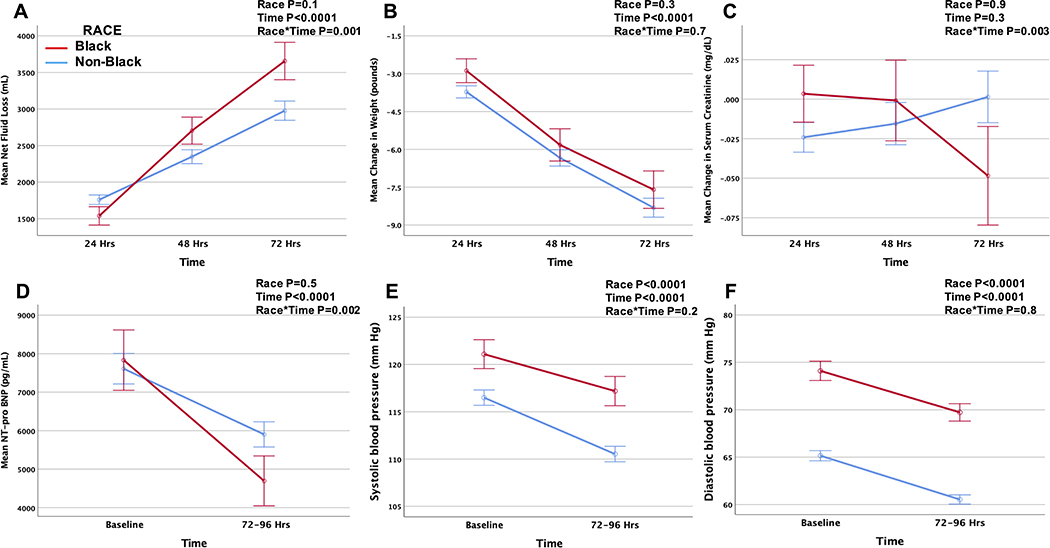
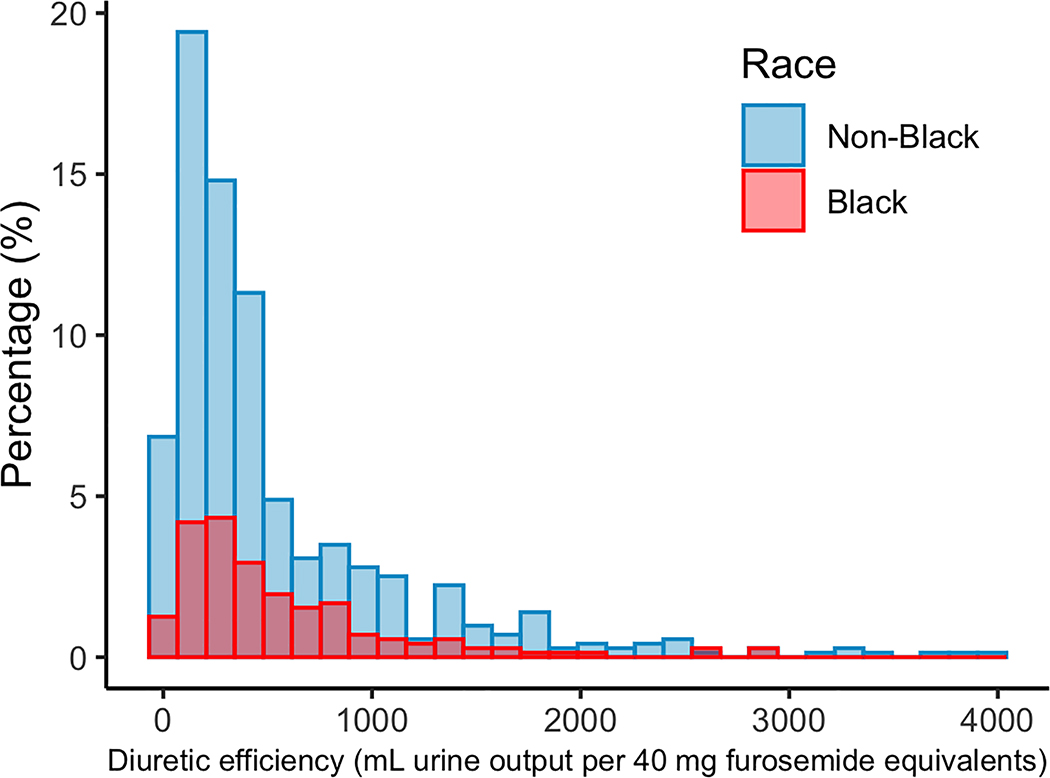
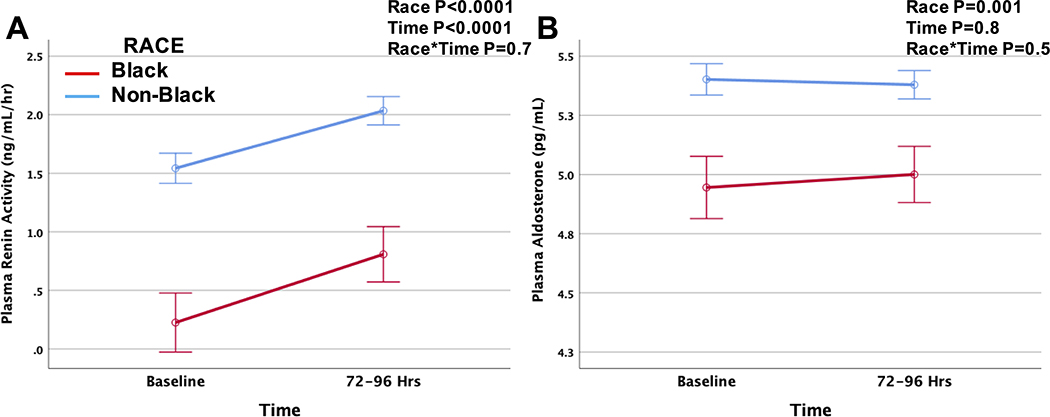
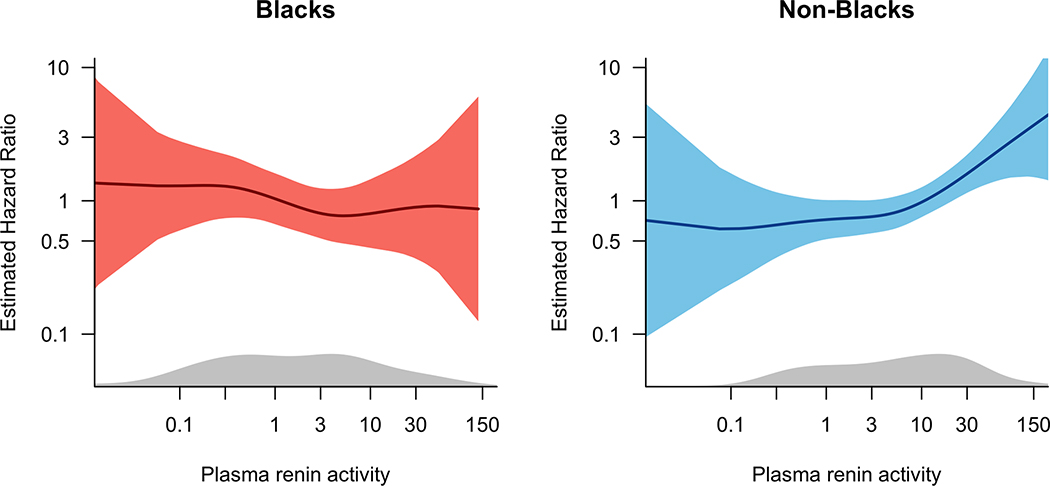
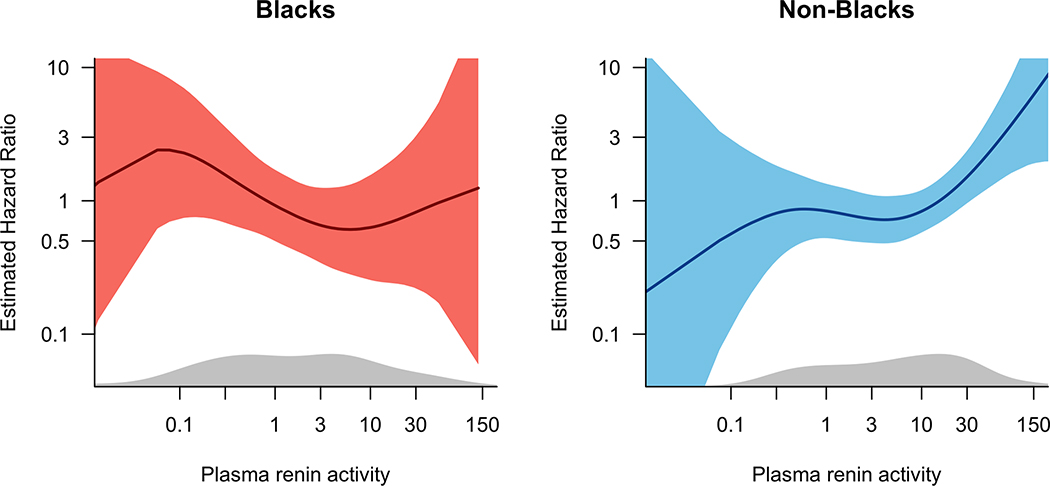
Results: Compared with nonblack patients, black patients were younger and more likely to have nonischemic heart failure. During the first 72 to 96 hours, there was greater fluid loss (P=0.001), decrease in NT-proBNP (N-terminal pro-B-type natriuretic peptide; P=0.002), and lower levels of PRA (P<0.0001) in black patients. Diuretic efficiency was higher in black than in nonblack patients (403 [interquartile range, 221-795] versus 325 [interquartile range, 154-698]; P=0.014). However, adjustment for baseline PRA attenuated the association between black race and diuretic efficiency. Over a median follow-up of 68 (interquartile range, 56-177) days, there was an increased risk of all-cause and heart failure-specific rehospitalization in nonblack patients with increasing levels of PRA, while the risk of rehospitalization was relatively constant across levels of PRA in black patients.
Conclusions: Higher diuretic efficiency in black patients with acute heart failure may be related to racial differences in activity of the renin-angiotensin-aldosterone system.
Keywords: disparities; diuretics; heart failure; humans; race factors; renin.
Figures
Similar articles
-
Decongestion strategies and renin-angiotensin-aldosterone system activation in acute heart failure.JACC Heart Fail. 2015 Feb;3(2):97-107. doi: 10.1016/j.jchf.2014.09.003. Epub 2014 Oct 31. JACC Heart Fail. 2015. PMID: 25543972 Free PMC article. Clinical Trial.
-
Relief and Recurrence of Congestion During and After Hospitalization for Acute Heart Failure: Insights From Diuretic Optimization Strategy Evaluation in Acute Decompensated Heart Failure (DOSE-AHF) and Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARESS-HF).Circ Heart Fail. 2015 Jul;8(4):741-8. doi: 10.1161/CIRCHEARTFAILURE.114.001957. Epub 2015 Jun 3. Circ Heart Fail. 2015. PMID: 26041600 Free PMC article. Clinical Trial.
-
Markers of decongestion, dyspnea relief, and clinical outcomes among patients hospitalized with acute heart failure.Circ Heart Fail. 2013 Mar;6(2):240-5. doi: 10.1161/CIRCHEARTFAILURE.112.969246. Epub 2012 Dec 18. Circ Heart Fail. 2013. PMID: 23250981 Free PMC article.
-
Trajectory of Decongestion and Mortality in Young Adults with Acute Heart Failure.Curr Probl Cardiol. 2023 Apr;48(4):101579. doi: 10.1016/j.cpcardiol.2022.101579. Epub 2022 Dec 30. Curr Probl Cardiol. 2023. PMID: 36592843 Review.
-
The management of acute heart failure and diuretic therapy.Am J Ther. 2009 Jan-Feb;16(1):93-7. doi: 10.1097/MJT.0b013e3181966c06. Am J Ther. 2009. PMID: 19142155 Review.
Cited by
-
Lipoprotein(a) and Heart Failure Among Black and White Participants in Atherosclerosis Risk in Communities Study, Framingham Offspring Study, and Multi-Ethnic Study of Atherosclerosis: The Pooling Project.J Am Heart Assoc. 2025 Jun 3;14(11):e038608. doi: 10.1161/JAHA.124.038608. Epub 2025 May 26. J Am Heart Assoc. 2025. PMID: 40417812 Free PMC article.
-
Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care.J Cardiovasc Dev Dis. 2023 Dec 5;10(12):486. doi: 10.3390/jcdd10120486. J Cardiovasc Dev Dis. 2023. PMID: 38132654 Free PMC article.
-
Understanding the Complexity of Heart Failure Risk and Treatment in Black Patients.Circ Heart Fail. 2020 Aug;13(8):e007264. doi: 10.1161/CIRCHEARTFAILURE.120.007264. Epub 2020 Aug 13. Circ Heart Fail. 2020. PMID: 32787445 Free PMC article. Review.
-
Racial Differences in Natriuresis: A Post Hoc Analysis of the ROSE-AHF Trial.JACC Heart Fail. 2022 Nov;10(11):876-878. doi: 10.1016/j.jchf.2022.08.019. JACC Heart Fail. 2022. PMID: 36328658 Free PMC article. No abstract available.
-
The Impact of Health Care Disparities on Patients With Heart Failure.J Card Fail. 2022 Jul;28(7):1169-1184. doi: 10.1016/j.cardfail.2022.04.008. Epub 2022 May 17. J Card Fail. 2022. PMID: 35595161 Free PMC article. Review.
References
-
- McDermott KW, Elixhauser A and Sun R. Trends in Hospital Inpatient Stays in the United States, 2005–2014 HCUP Statistical Brief #225. June 2017. Agency for Healthcare Research and Quality, Rockville, MD: www.hcup-us.ahrq.gov/reports/statbriefs/sb225-Inpatient-US-Stays-Trends.pdf.
-
- Kiernan MS, Stevens SR, Tang WHW, Butler J, Anstrom KJ, Birati EY, Grodin JL, Gupta D, Margulies KB, LaRue S, Dávila-Román VG, Hernandez AF and de las Fuentes L. Determinants of Diuretic Responsiveness and Associated Outcomes During Acute Heart Failure Hospitalization: An Analysis From the NHLBI Heart Failure Network Clinical Trials. Journal of Cardiac Failure. 2018;24:428–438. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
