

Case Reports
doi: 10.1007/s00401-020-02190-2.
Epub 2020 Jul 8.
Microvascular injury and hypoxic damage: emerging neuropathological signatures in COVID-19
Affiliations
- PMID: 32638079
- PMCID: PMC7340758
- DOI: 10.1007/s00401-020-02190-2
Item in Clipboard
Case Reports
Microvascular injury and hypoxic damage: emerging neuropathological signatures in COVID-19
Acta Neuropathol.
2020 Sep.
No abstract available
Conflict of interest statement
The authors declare no conflict of interest.
Figures
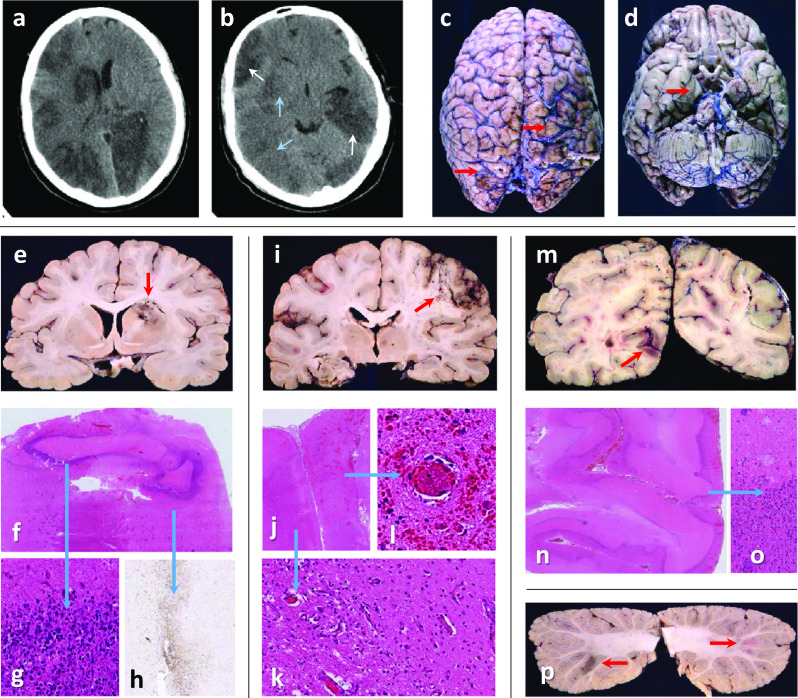
Case 1: a, b Head-CT shows recent (blue arrows) and established (white arrows) multifocal infarcts. c Rusty discolouration (red arrows) on brain surface. d Right uncal grooving (red arrow). e Bilateral acute and subacute watershed infarcts in the anterior-MCA and MCA–PCA territories and a subacute infarct in the right lentiform nucleus (red arrow). f, g Dense inner rim of degenerating neutrophils (blue arrow) and h, an outer rim (blue arrow) of macrophages (CD68). i, j Macroscopy and microscopy of confluent infarcts across the right MCA territory (acute and subacute, red arrow). k Infarcts are ischaemic, with granulation tissue and macrophages (blue arrow), or l, with perivascular haemorrhages and fibrin thrombi (blue arrow). m Bilateral acute and subacute infarcts in the PCA territories (both occipital lobes (red arrow), and i left hippocampus and thalamus. n, o Frequently, subacute infarcts show prominent leukocytoclastic reaction (blue arrow). p Multiple subacute cortical infarcts in both cerebellar hemispheres (red arrows)

Case 2: a MRI brain (FLAIR image) shows leukoaraiosis and high signal intensity in the right (red arrow) but not left (white arrow) intraparietal sulcus. b Microhaemorrhage on the left (red arrow), but no gross leptomeningeal pathology. c, d Histology shows mild leptomeningeal lymphohistiocytic inflammation in the right (d), but not left (c) intraparietal sulcus. e Arrows point to microhaemorrhages (T2*weighted MRI), f macroscopically (red arrows) and g, h microscopically corresponding to acute and subacute white matter microbleeds. i Small acute infarcts (DWI MRI, black arrows), j macroscopically corresponding to white matter lesions (ø1-4 mm, red arrows). k Histologically, some are classic acute and subacute microinfarcts (red arrow), l whilst others contain haemosiderin-laden macrophages, m shown with Perls staining. n CD68 accentuates many more lesions than evident macroscopically or on MRI. o Unremarkable blood vessels are seen within some of the white matter microlesions (CD34 immunostaining). p Swollen axons (indicating damage) on neurofilament (SMI31) immunostaining q but no demyelination (myelin basic protein (SMI94) immunostaining). r Macroscopic and microscopic examination (inset in r shows macrophage-rich necrosis) reveal bilateral subacute pallidal infarcts. s Occasional subacute microinfarcts in the cortex (ø1–5 mm), some with haemorrhagic transformation (inset in s). t High MRI T1 signal foci (white arrow) in the cerebellum correspond histologically to u subacute infarct, v fresh leptomeningeal haemorrhages and (not shown) non-haemorrhagic white matter microlesions. w Several chronic infarcts and microinfarcts (likely embolic) in cerebellar cortex and right thalamus (not shown)
References
-
- Bryce C, Grimes Z, Pujadas E, Ahuja S, Beasley MB, Albrecht R, Hernandez T, Stock A, Zhao Z, Al Rasheed M et al (2020) Pathophysiology of SARS-CoV-2: targeting of endothelial cells renders a complex disease with thrombotic microangiopathy and aberrant immune response. The Mount Sinai COVID-19 autopsy experience. medRxiv: 2020.2005.2018.20099960. 10.1101/2020.05.18.20099960
-
- Lorusso R, Gelsomino S, Parise O, Di Mauro M, Barili F, Geskes G, Vizzardi E, Rycus PT, Muellenbach R, Mueller T, et al. Neurologic injury in adults supported with veno-venous extracorporeal membrane oxygenation for respiratory failure: findings from the extracorporeal life support organization database. Crit Care Med. 2017;45:1389–1397. doi: 10.1097/ccm.0000000000002502. - DOI - PubMed
-
- Magro C, Mulvey JJ, Berlin D, Nuovo G, Salvatore S, Harp J, Baxter-Stoltzfus A, Laurence J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Translational research : the journal of laboratory and clinical medicine. 2020;220:1–13. doi: 10.1016/j.trsl.2020.04.007. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
