

Impact of Unannounced Standardized Patient Audit and Feedback on Care, Documentation, and Costs: an Experiment and Claims Analysis
- PMID: 32638322
- PMCID: PMC7859004
- DOI: 10.1007/s11606-020-05965-1
Impact of Unannounced Standardized Patient Audit and Feedback on Care, Documentation, and Costs: an Experiment and Claims Analysis
Abstract
Background: Meaningful variations in physician performance are not always discernible from the medical record.
Objective: We used unannounced standardized patients to measure and provide feedback on care quality and fidelity of documentation, and examined downstream effects on reimbursement claims.
Design: Static group pre-post comparison study conducted between 2017 and 2019.
Setting: Fourteen New Jersey primary care practice groups (22 practices) enrolled in Horizon BCBS's value-based program received the intervention. For claims analyses, we identified 14 additional comparison practice groups matched on county, practice size, and claims activity.
Participants: Fifty-nine of 64 providers volunteered to participate.
Intervention: Unannounced standardized patients (USPs) made 217 visits portraying patients with 1-2 focal conditions (diabetes, depression, back pain, smoking, or preventive cancer screening). After two baseline visits to a provider, we delivered feedback and conducted two follow-up visits.
Measurements: USP-completed checklists of guideline-based provider care behaviors, visit audio recordings, and provider notes were used to measure behaviors performed and documentation errors pre- and post-feedback. We also compared changes in 3-month office-based claims by actual patients between the intervention and comparison practice groups before and after feedback.
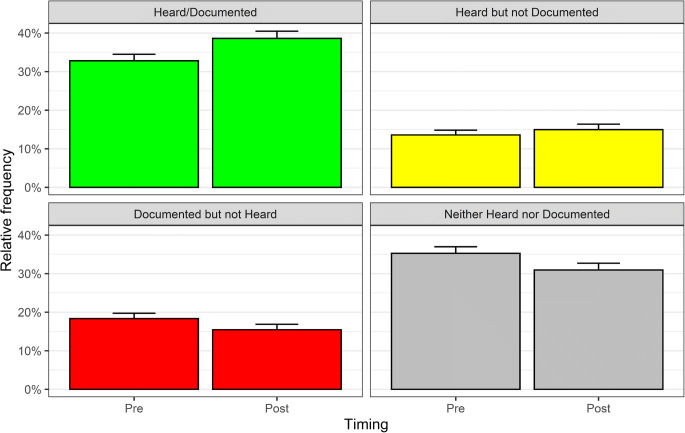
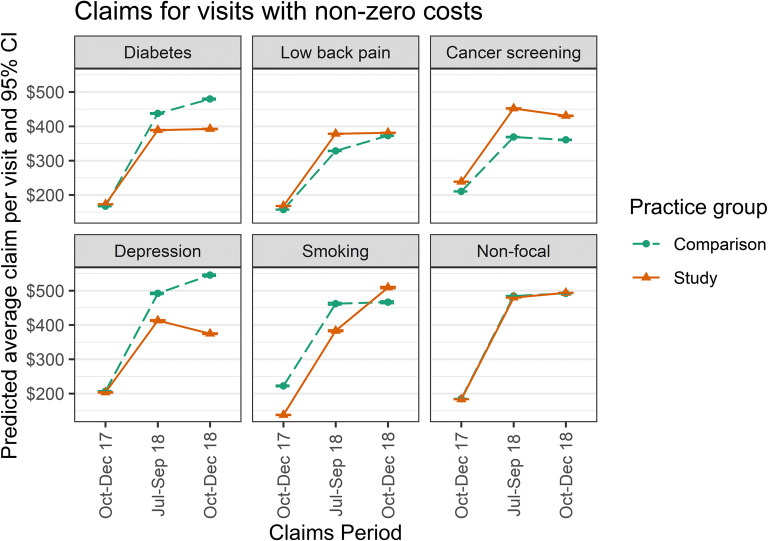
Results: Expected clinical behaviors increased from 46% to 56% (OR = 1.53, 95% CI 1.29-1.83, p < 0.0001), with significant improvements in smoking cessation, back pain, and depression screening. Providers were less likely to document unperformed tasks after (16%) than before feedback (18%; OR = 0.74, 95% CI 0.62 to 0.90, p = 0.002). Actual claim costs increased significantly less in the study than comparison group for diabetes and depression but significantly more for smoking cessation, cancer screening, and low back pain.
Limitations: Self-selection of participating practices and lack of access to prescription claims.
Conclusion: Direct observation of care identifies hidden deficits in practice and documentation, and with feedback can improve both, with concomitant effects on costs.
Keywords: cost of care; directly observed care; health services research; quality improvement; unannounced standardized patients.
Conflict of interest statement
Schwartz, Weiner, and Spiro conducted this work as employees and board members of the Institute for Practice and Provider Performance Improvement, Inc. Peskin is an employee of Horizon Blue Cross Blue Shield of New Jersey. Neither Peskin nor Horizon was compensated for their participation.
Figures
References
-
- Stange KC, Zyzanski SJ, Jaen CR, et al. Illuminating the 'black box'. A description of 4454 patient visits to 138 family physicians. J Fam Pract. 1998;46(5):377–389. - PubMed
-
- National Center for Quality Assurance. http://www.ncqa.org/HEDISQualityMeasurement/PerformanceMeasurement.aspx, 2013.
-
- Agency for Healthcare Research and Quality. CAHPS clinician & group surveys. Available at: https://cahps.ahrq.gov/Surveys-Guidance/CG/index.html. Last accessed May 10, 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
