

A Randomized Trial of a Multifactorial Strategy to Prevent Serious Fall Injuries
- PMID: 32640131
- PMCID: PMC7421468
- DOI: 10.1056/NEJMoa2002183
A Randomized Trial of a Multifactorial Strategy to Prevent Serious Fall Injuries
Abstract
Background: Injuries from falls are major contributors to complications and death in older adults. Despite evidence from efficacy trials that many falls can be prevented, rates of falls resulting in injury have not declined.
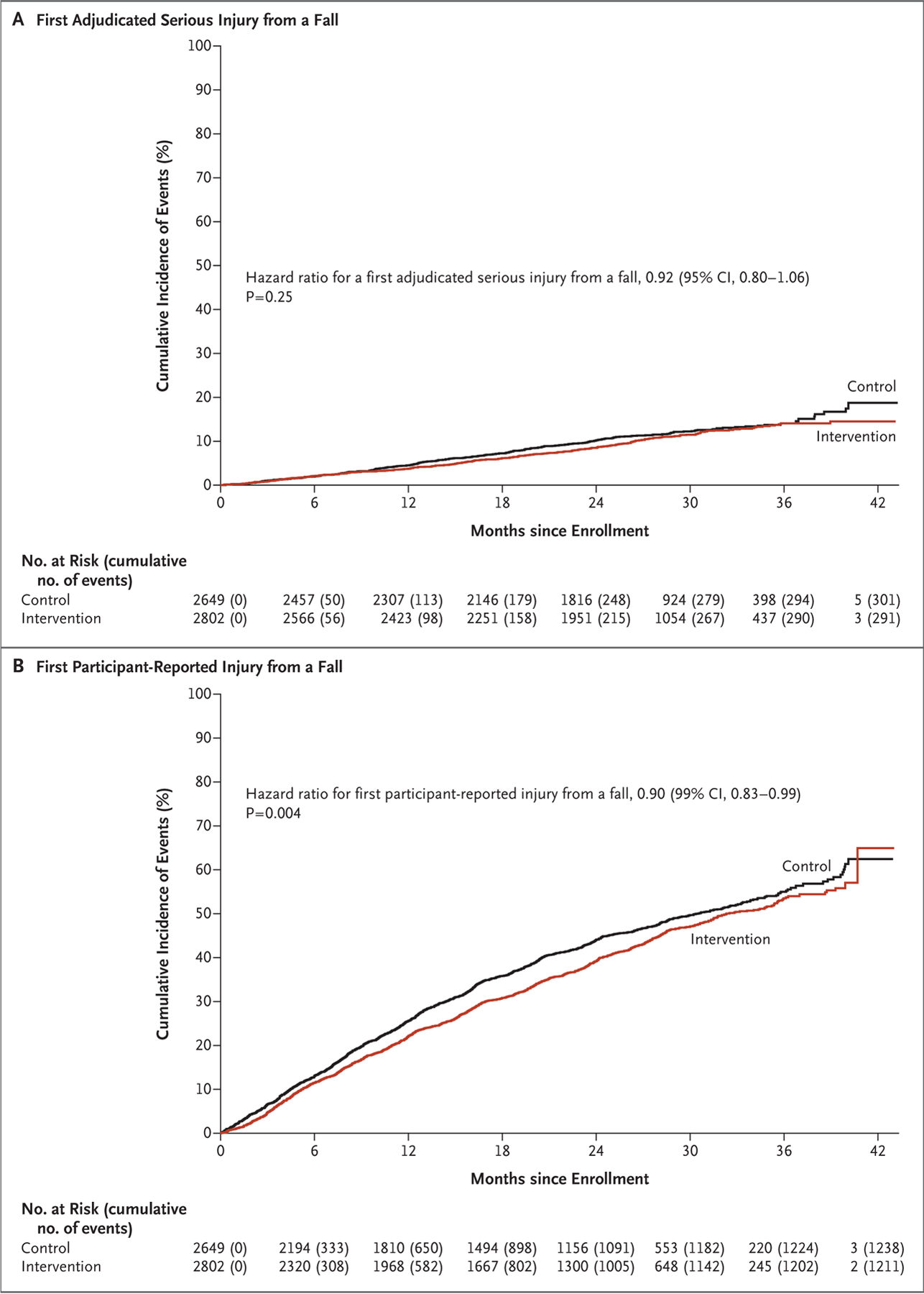
Methods: We conducted a pragmatic, cluster-randomized trial to evaluate the effectiveness of a multifactorial intervention that included risk assessment and individualized plans, administered by specially trained nurses, to prevent fall injuries. A total of 86 primary care practices across 10 health care systems were randomly assigned to the intervention or to enhanced usual care (the control) (43 practices each). The participants were community-dwelling adults, 70 years of age or older, who were at increased risk for fall injuries. The primary outcome, assessed in a time-to-event analysis, was the first serious fall injury, adjudicated with the use of participant report, electronic health records, and claims data. We hypothesized that the event rate would be lower by 20% in the intervention group than in the control group.
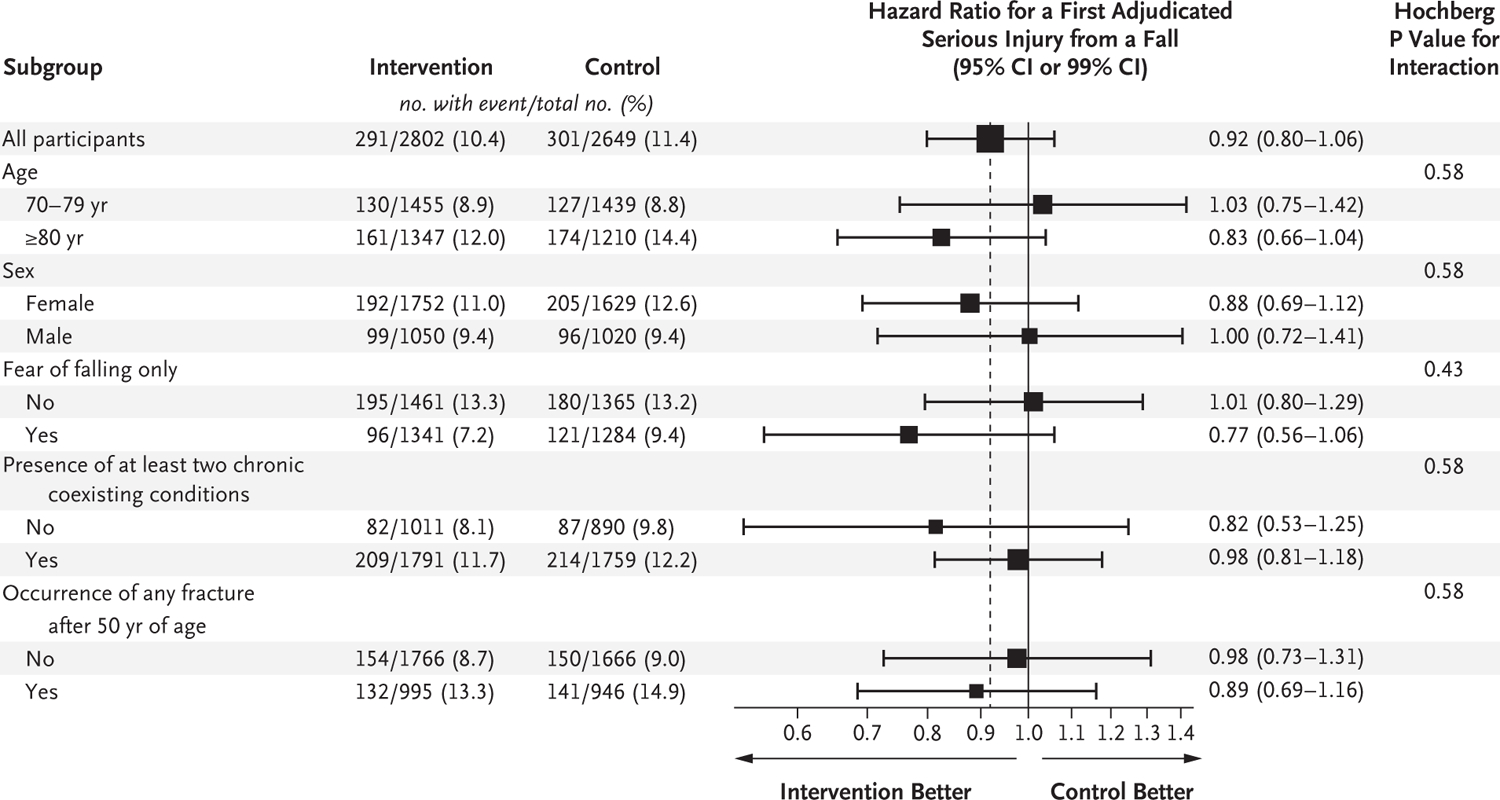
Results: The demographic and baseline characteristics of the participants were similar in the intervention group (2802 participants) and the control group (2649 participants); the mean age was 80 years, and 62.0% of the participants were women. The rate of a first adjudicated serious fall injury did not differ significantly between the groups, as assessed in a time-to-first-event analysis (events per 100 person-years of follow-up, 4.9 in the intervention group and 5.3 in the control group; hazard ratio, 0.92; 95% confidence interval [CI], 0.80 to 1.06; P = 0.25). The rate of a first participant-reported fall injury was 25.6 events per 100 person-years of follow-up in the intervention group and 28.6 events per 100 person-years of follow-up in the control group (hazard ratio, 0.90; 95% CI, 0.83 to 0.99; P = 0.004). The rates of hospitalization or death were similar in the two groups.
Conclusions: A multifactorial intervention, administered by nurses, did not result in a significantly lower rate of a first adjudicated serious fall injury than enhanced usual care. (Funded by the Patient-Centered Outcomes Research Institute and others; STRIDE ClinicalTrials.gov number, NCT02475850.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
A Multifactorial Trial to Prevent Serious Fall Injuries.N Engl J Med. 2020 Oct 1;383(14):1395. doi: 10.1056/NEJMc2026944. N Engl J Med. 2020. PMID: 32997923 No abstract available.
-
Strategies to Prevent Serious Fall Injuries: A Commentary on Bhasin et al. A Randomized Trial of a Multifactorial Strategy to Prevent Serious Fall Injuries. N Engl J Med. 2020;383(2):129-140.Adv Geriatr Med Res. 2021;3(1):e210002. doi: 10.20900/agmr20210002. Epub 2020 Nov 14. Adv Geriatr Med Res. 2021. PMID: 33283207 Free PMC article.
References
-
- Health, United States, 2016: with chartbook on long-term trends in health. Hyattsville, MD: National Center for Health Statistics, May 2017. - PubMed
-
- Bergen G, Stevens MR, Burns ER. Falls and fall injuries among adults aged ≥65 years — United States, 2014. MMWR Morb Mortal Wkly Rep 2016;65:993–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- 5U01AG048270/PCORI/Patient-Centered Outcomes Research Institute/United States
- K08 AG050808/AG/NIA NIH HHS/United States
- P30 AG028747/AG/NIA NIH HHS/United States
- P30 AG024824/AG/NIA NIH HHS/United States
- U24 AG059624/AG/NIA NIH HHS/United States
- P30 AG021342/AG/NIA NIH HHS/United States
- P30 AG028748/AG/NIA NIH HHS/United States
- UL1 TR000142/TR/NCATS NIH HHS/United States
- P30 AG028741/AG/NIA NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- P30 AG024832/AG/NIA NIH HHS/United States
- 5U01AG048270/AG/NIA NIH HHS/United States
- P30 AG021332/AG/NIA NIH HHS/United States
- K07 AG043587/AG/NIA NIH HHS/United States
- P30 AG024827/AG/NIA NIH HHS/United States
- U01 AG048270/AG/NIA NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- P30 AG031679/AG/NIA NIH HHS/United States
- UL1 TR000114/TR/NCATS NIH HHS/United States
- KL2 TR000113/TR/NCATS NIH HHS/United States