

Do primary and secondary care doctors have a different experience and perception of cross-level clinical coordination? Results of a cross-sectional study in the Catalan National Health System (Spain)
- PMID: 32640991
- PMCID: PMC7346358
- DOI: 10.1186/s12875-020-01207-9
Do primary and secondary care doctors have a different experience and perception of cross-level clinical coordination? Results of a cross-sectional study in the Catalan National Health System (Spain)
Abstract
Background: Clinical coordination across care levels is a priority for health systems around the world, especially for those based on primary health care. The aim of this study is to analyse the degree of clinical information and clinical management coordination across healthcare levels in the Catalan national health system experienced by primary (PC) and secondary care (SC) doctors and explore the associated factors.
Methods: Cross-sectional study based on an online survey using the self-administered questionnaire COORDENA-CAT.
Data collection: October-December 2017.
Study population: PC and SC (acute and long term) doctors of the Catalan national health system. Participation rate was 21%, with a sample of 3308 doctors.
Outcome variables: cross-level clinical information coordination, clinical management coordination, and perception of cross-level coordination within the area. Explanatory variables: socio-demographic, employment characteristics, attitude towards job, type of area (according to type of hospital and management), interactional factors, organizational factors and knowledge of existing coordination mechanisms. Stratification variable: level of care. Descriptive and multivariate analysis by logistic regression.
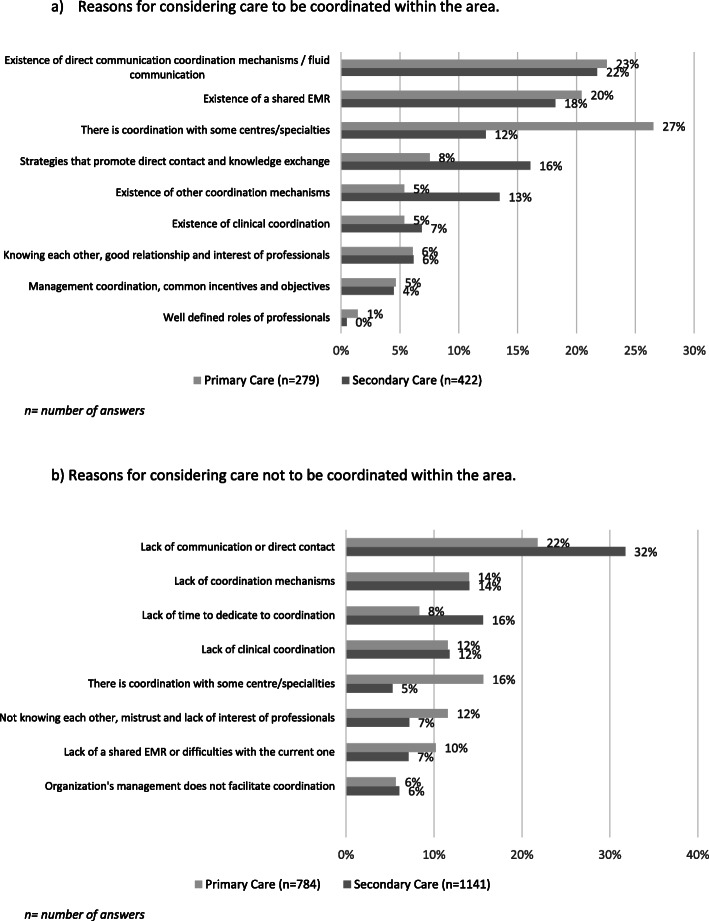
Results: The degree of clinical coordination experienced across levels of care was high for both PC and SC doctors, although PC doctors experienced greater exchange and use of information and SC doctors experienced greater consistency of care. However, only 32.13% of PC and 35.72% of SC doctors found that patient care was coordinated across care levels within their area. In both levels of care, knowing the doctors of the other level, working in an area where the same entity manages SC and majority of PC, and holding joint clinical case conferences were factors positively associated with perceiving high levels of clinical coordination. Other associated factors were specific to the care level, such as being informed of a patient's discharge from hospital for PC doctors, or trusting in the clinical skills of the other care level for SC doctors.
Conclusions: Interactional and organizational factors are positively associated with perceiving high levels of clinical coordination. Introducing policies to enhance such factors can foster clinical coordination between different health care levels. The COORDENA questionnaire allows us to identify fields for improvement in clinical coordination.
Keywords: Clinical coordination across care levels; Health systems research; Integrated care; Questionnaire.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Corral L, Borao M, Jorge RJ, García J. The patient and the crossing between primary and hospital care. Systematic review of trials for the implementation of tools for integration in Spain. An Sist Sanit Navar. 2017;40(3):443–459. - PubMed
-
- Lewis R, Rosen R, Goodwin N, Dixon J. Where next for integrated care organisations in the English NHS? The Nuffield trust. 2010.
-
- Vargas I, Vázquez ML. Redes Integradas de Servicios de Salud: ¿solución o problema? Rev ciencias la salud. 2006;4(1):5–9.
-
- Ovretveit J. Does clinical coordination improve quality and save money? Heal Found. 2011;1(June):1–21.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
