

A systematic review and time-response meta-analysis of the optimal timing of elective caesarean sections for best maternal and neonatal health outcomes
- PMID: 32641019
- PMCID: PMC7341650
- DOI: 10.1186/s12884-020-03036-1
A systematic review and time-response meta-analysis of the optimal timing of elective caesarean sections for best maternal and neonatal health outcomes
Abstract
Background: The rate of caesarean sections (CS) has increased in the last decades to about 30% of births in high income countries. Many CSs are electively planned without an urgent medical reason for mother or child. An early CS though may harm the newborn. Our aim was to evaluate the gestational time point after the 37 + 0 week of gestation (WG) (after prematurity = term) of performing an elective CS with the lowest morbidity for mother and child by assessing the time course from 37 + 0 to 42+ 6 WG.
Methods: We performed a systematic literature search in MEDLINE, EMBASE, CENTRAL and CINAHL in November 2018. We included studies that compared different time points of elective CS at term no matter the reason for elective CS. Our primary outcomes were the rate of admissions to the neonatal intensive care unit (NICU), neonatal death and maternal death in early versus late term elective CS. Various binary and dose response random effects meta-analyses were performed.
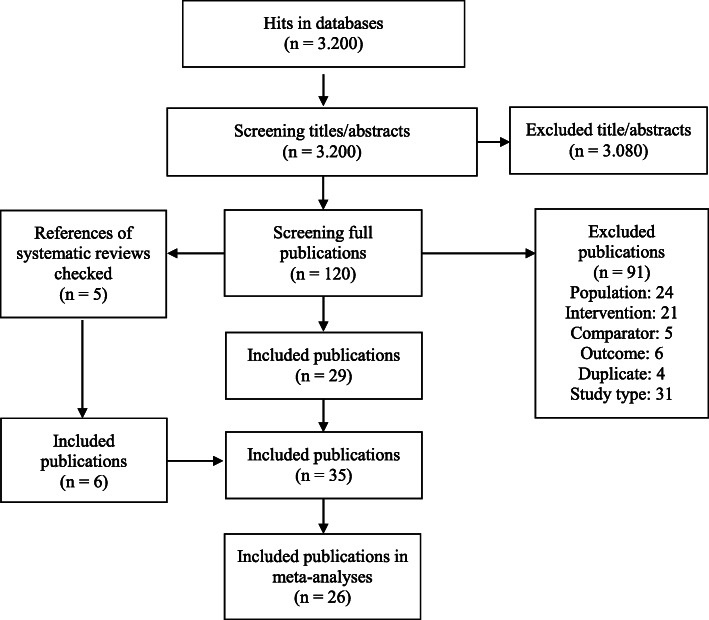
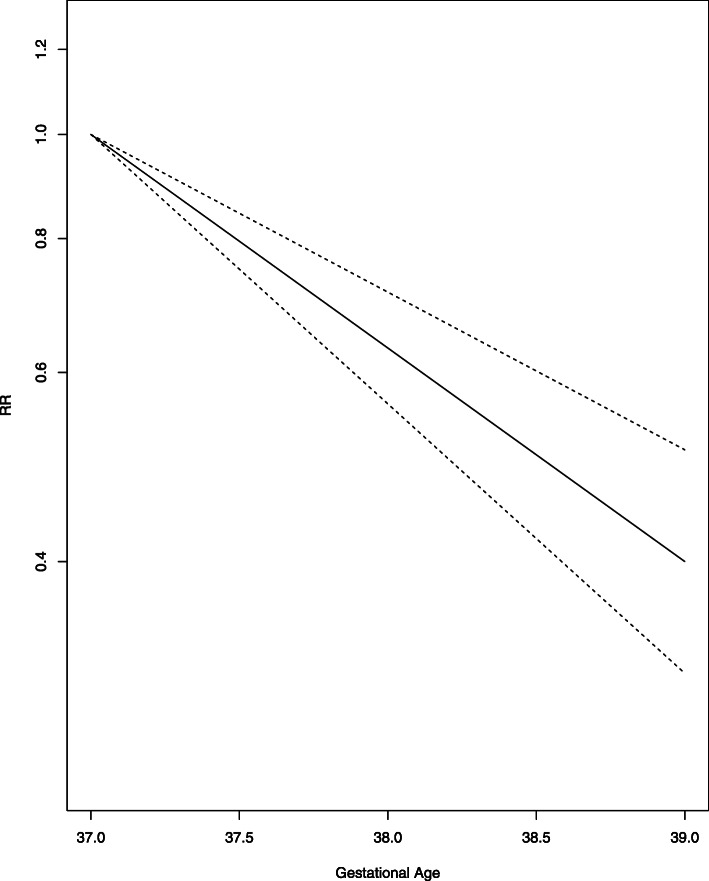
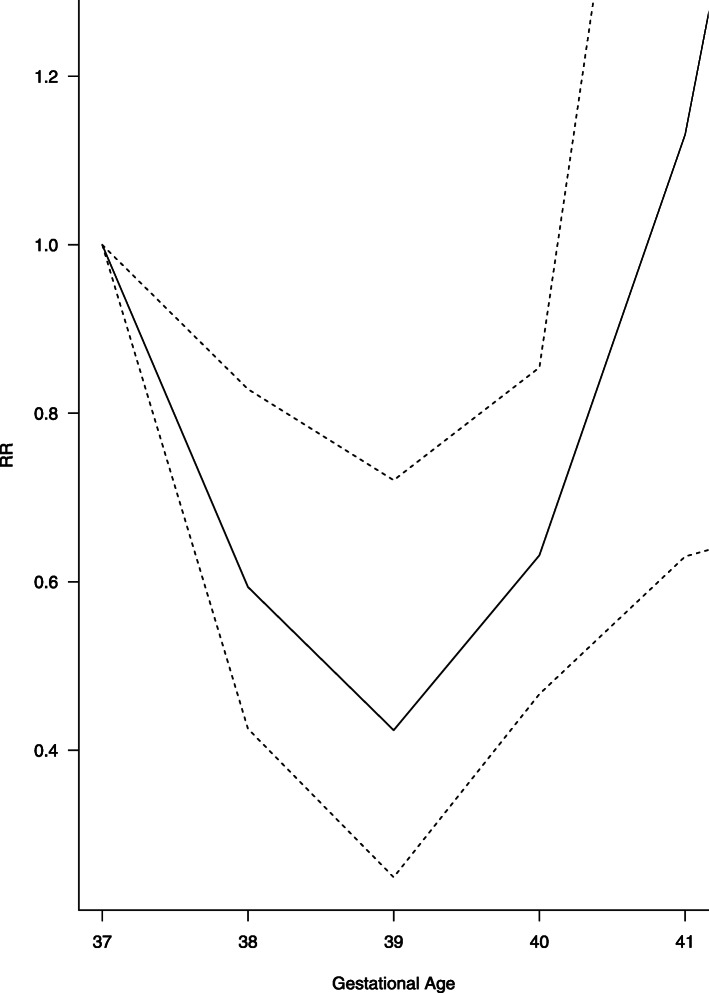
Results: We identified 35 studies including 982,749 women. Except one randomised controlled trial, all studies were cohort studies. We performed a linear time-response meta-analysis on the primary outcome NICU admission on 14 studies resulting in a decrease of the relative risk (RR) to 0.63 (95% CI 0.56, 0.71) from 37 + 0 to 39 + 6 WG. RR for neonatal death showed a decrease to 39 + (0-6) WG (RR 0.59 95% CI 0.43 to 0.83) and increase from then on (RR 2.09 95% CI 1.18 to 3.70) assuming a U-shape course and using a cubic spline model for meta-analysis of four studies. We only identified one study analyzing maternal death resulting in RR of 0.38 (95% CI 0.04 to 3.40) for 37 + 0 + 38 + 6 WG versus ≥39 + 0 WG.
Conclusion: Our systematic review showed that elective CS (primary and repeated) before the 39 + 0 WG lead to more NICU admissions and neonatal deaths, although death is rare and increases again after 39 + 6 WG. We did not find enough evidence on maternal outcomes. There is a need for more research, considering maternal outcomes to provide a balanced decision between neonatal and maternal health.
Systematic review registration: Registered in PROSPERO (CRD42017078231).
Keywords: Elective caesarean section; Gestational age; Maternal morbidity; Neonatal intensive care unit; Neonatal morbidity; Term birth; Time-response meta-analysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO Appropriate technology for birth. Lancet. 1985;326(8452):436–437. - PubMed
-
- Betrán AP, Merialdi M, Lauer JA, Bing-Shun W, Thomas J, Look PV, et al. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol. 2007;21(2):98–113. - PubMed
-
- Ye J, Betrán AP, Vela MG, Souza JP, Zhang J. Searching for the optimal rate of medically necessary cesarean delivery. Birth. 2014;41(3):237–244. - PubMed
-
- Knight HE, Gurol-Urganci I, van der Meulen JH, Mahmood TA, Richmond DH, Dougall A, et al. Vaginal birth after caesarean section: a cohort study investigating factors associated with its uptake and success. BJOG Int J Obstet Gynaecol. 2014;121(2):183–192. - PubMed
-
- MacDorman M, Declercq E, Menacker F. Recent trends and patterns in cesarean and vaginal birth after cesarean (VBAC) deliveries in the United States. Clin Perinatol. 2011;38(2):179–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
