

Comparative effectiveness and cost-efficiency of surgical approaches for thymectomy
- PMID: 32641277
- PMCID: PMC7816338
- DOI: 10.1016/j.surg.2020.04.037
Comparative effectiveness and cost-efficiency of surgical approaches for thymectomy
Abstract
Background: We compared the clinical outcomes and cost-efficiency of surgical approaches (sternotomy-open, video assisted thoracoscopic surgery, and robotic assisted thoracic surgery) for thymectomy.
Methods: This is a retrospective review of 220 consecutive patients who underwent thymectomy between January 1, 2007, and January 31, 2017. Surgical approach was determined by the surgeon, but we only included cases that could be resected using any of the 3 approaches.
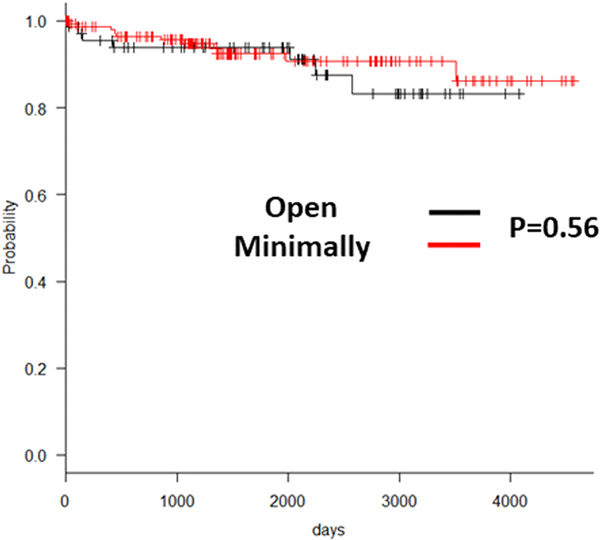
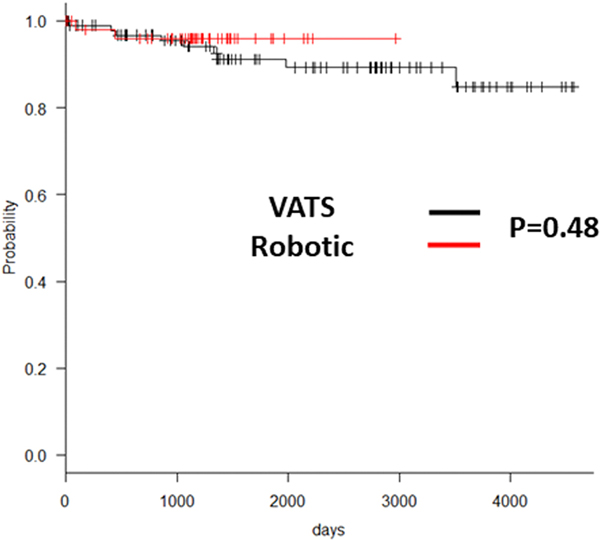
Results: Open approach was used in 69 patients, whereas minimally invasive technique was used in 151 (97, video assisted thoracoscopic surgery; 54, robotic assisted thoracic surgery). Open surgery was associated with greater total hospital cost ($22,847 ± $20,061 vs $14,504 ± $10,845, P < .001). Open group also revealed longer duration of intensive care unit (1.2 ± 2.8 vs 0.2 ± 1.3 days, P < .001) and hospital stay (4.3 ± 4.0 vs 2.0 ± 2.6 days, P < .001). There were no differences in major adverse clinical outcomes. Long-term recurrence-free survival after resection of thymoma was similar between the groups.
Conclusion: Minimally invasive techniques were equally efficacious compared with the open approach in the resection of the thymus. Additionally, their use was associated with decreased hospital duration of stay and reduced cost. Hence the use of minimally invasive approaches should be encouraged in the resection of thymus.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
COI/ Disclosures
The authors have no related conflicts of interest to declare.
Figures
References
-
- Davenport E, Malthaner RA. The role of surgery in the management of thymoma: a systematic review. Ann Thorac Surg. 2008;86(2):673–84. - PubMed
-
- Venuta F, Rendina EA, Anile M, de Giacomo T, Vitolo D, Coloni GF. Thymoma and thymic carcinoma. Gen Thorac Cardiovasc Surg. 2012;60(1):1–12. - PubMed
-
- Ye B, Tantai JC, Ge XX, Li W, Feng J, Cheng M, et al. Surgical techniques for early-stage thymoma: video-assisted thoracoscopic thymectomy versus transsternal thymectomy. J Thorac Cardiovasc Surg. 2014;147(5):1599–603. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
